
Coca-Cola, often referred as Coke, is a carbonated soft drinksold in stores, restaurants,
and vending machines in more than 200 countries. It is produced by The Coca-Cola Company of Atlanta,
Georgia.
It was invented in the late 19th century by John Pemberton, but Coca-Cola was bought out by businessman
Asa Griggs Candler, whose marketing tactics led Coke to its dominance of the world soft-drink market
throughout the 20th century.
Formula
The Coca-Cola formula is The Coca-Cola Company's secret recipe for Coca-Cola. As a publicity, marketing,
and intellectual property protection strategy, the company presents the formula as a closely held trade secret
known only to a few employees.
Coca-Cola was originally a coca-based medicine (coca leaves were used in its preparation),which claimed to
alleviate headaches and to be a "brain and nerve tonic". In 1903 Coca-Cola removed cocaine from the formula,
started using caffeine and started dropping all the medicinal claims.
Today published versions say it contains water, carbon dioxide, sugar or high fructose corn syrup, caramel color,
caffeine, phosphoric acid, lime extract, vanilla, and glycerin.
Cola effects
Injuries derived from an excessive consumption of Cola are quite well known today, expecially because of its
content in caffeine that is a potent psychostimulant probably acting at adenosine receptors and which can
cause physical dependence, its high acidity levels and the considerable presence of sugar and fructose
corn syrup.
Here are presented some of the less known Cola effects:
• Seizures and hyponatriemia.
• Tooth erosion.
• Loss of sperm motility and spermicidal effects.
• Changes in behavior and endocrine system.
Chronic intake of caffeine containing cola has similar effects to that of caffeine: an increase in locomotor
activity and anxiety and a partial anti-depressive effect.
These alternations might be associated with observed endocrine changes in testosterone and oestradiol levels.
• Fatty liver desease.
• Osteoporosis in postmenopausal women.
While pathways involved in most of the previous deseases are still quite obscure today and need more
investigations, more answers can be found to explain fatty liver desease and osteoporosis.
Fatty liver disease
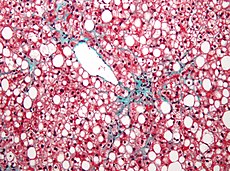
Fatty liver, also known as fatty liver disease (FLD), is a reversible condition where large vacuoles of triglyceride
fat accumulate in liver cells via the process of steatosis.
Little is known about dietary habits and their relationships with liver disease in nonalcoholic fatty liver disease
(NAFLD) patients, particularly in the absence of obesity, diabetes or hyperlipidemia. Anyway recent studies
have shown that Coke can be a cause of fatty liver in patients without risk factors. NAFLD can progressively
grow into NASH (Nonalcoholic steatohepatitis).
Recent evidence suggests that consumption of sugar-sweetened soft drink like Coke is associated with the
risk of obesity and diabetes because they contain large amounts of high-fructose corn syrup.
In addition, soft drinks contain caramel colouring, which is rich in advanced glycation end products
that might increase insulin resistance and inflammation. Such diets have also caused increases in
hepatic lipid peroxidation and activation of inflammatory
pathways in the liver of rats. Fructose consumption can cause progressive liver disease in humans.
Sugars and colourants may promote insulin resistance, lipid peroxidation and hepatic inflammation,
and are a source of glycation end products.
Fructose can also increase triglyceride levels, de novo synthesis of fatty acids, hyperuricemia and insulin resistance.
The triglyceride response to fructose ingestion appears to depend on whether a person is carbohydrate-sensitive
or insulin-resistant . Fructose, especially high-fructose corn syrup, is now used extensively in cola beverages.
After absorption in the small bowel, fructose is transported via the portal vein to the liver, where it is metabolized
by fructokinase to fructose-1-phosphate. This molecule is cleaved by aldolase to form glycerone phosphate
and glyceraldehyde-3-phosphate, both of which can be further metabolized in the glycolytic pathway. An increase
in serum triglycerides and, ultimately, increased low-density lipoprotein cholesterol concentration may result
from enhanced fatty acid synthesis, increased esterification of fatty acids and increased very low-density
lipoprotein secretion.

Aspartame is absorbed from the intestine and metabolized by the liver to form phenylalanine,
aspartic acid and methanol. This process causes mitochondrial dysfunction and ATP depletion, which contribute
to accumulation of fat. Formaldehyde converted from the free methyl alcohol accumulates in the cells and damages
mitochondrial DNA, with most toxicity effects occurring in the liver.
Finally, the effect of caramel colourant has been incriminated as a cause of elevated liver enzymes and may be
a potential source of advanced glycation end product, which may promote insulin resistance
and can be proinflammatory.
Osteoporosis
Osteoporosis and related fractures represent one of the major public health problems. With the aging
of the population, the health care burden from fractures is expected to increase dramatically during the next
few decades. The lifetime risk of fracture exceeds 40% for women and 13% for men, and hip fractures have been
associated with an excess mortality of up to 20%.
It is, therefore, of great importance to identify modifiable risk factors for osteoporosis. Increasingly, numerous
dietary behaviors and components have been identified as important contributors to the risk of loss of bone
mineral density (BMD) with aging. Several studies have examined the association between carbonated
beverages and fracture, hypocalcemia, or BMD in different groups of people like children, young girls,
postmenopausal women, athletes. But the results are controversial: in some cases a relationship was found,
other studies did not confirmed that hypothesis.
Coke requires a different treatment. In fact there are several reasons to hypothesize that colas may be
associated with lower BMD.
Recent studies have shown consistent associations between cola consumption and low BMD in women.
It is not clear why females would be more sensitive to the effects of cola than are males. Girls and women
have smaller bones, are at higher risk of osteoporosis, and may be more sensitive to nutritional insult.
It was suggested that greater physical activity and sometimes higher calcium intakes (generally men in our
population had similar calcium intakes compared with the women) in boys may protect them against the negative
effects of soft drinks. Hormonal interactions may also contribute to these differing results by sex.
Caffeine is an ingredient in most colas and has been identified as a risk factor for osteoporosis. In epidemiological
studies, intake of caffeine was associated with higher levels of oestrogens and lower free testosterone in
post-menopausal women.
However, even if caffeine likely contributes to lower BMD, significant results were also observed for
decaffeinated cola, suggesting that caffeine does not explain these results.
Colas contain phosphoric acid whereas other carbonated soft drinks (with some exceptions) do not.
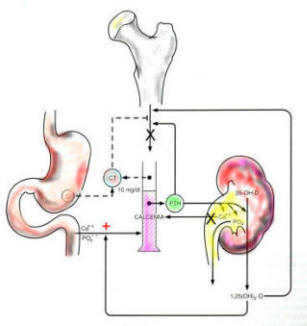
Deleterious effect of phosphoric acid has been proposed. Theoretically, diets high in phosphorus and low in
calcium lead to a reduction in serum calcium, stimulating parathyroid hormone (PTH), which, in turn, causes bone
resorption and returns serum calcium to homeostatic concentrations.
Although it was suggested that the amount of phosphoric acid in cola is insufficient to cause this imbalance,
it remains unclear whether regular exposure to phosphoric acid without exposure to calcium or other beneficial
nutrients slowly affects bone remodeling and causes bone loss over time.
High dietary phosphorus was shown to cause bone loss in animals . For example in one study, cola was given to
immature and adult rats and found that both developed significant hypercalciuria and hyperphosphaturia; the older
animals also developed hyperparathyroidism.
It is less clear how regular use of a beverage containing a dose of phosphoric acid, with no calcium
forming or neutralizing components, may affect BMD over a long-term exposure.
In addition to calciuric effects of high phosphorus and low calcium combinations, phosphoric acid present in the
gut may form a complex with dietary calcium to block its absorption. It is possible that this may reduce the calciuric
effect but still have a negative effect on bone by reducing total calcium availability.
It has also been suggested that the high fructose corn syrup used to sweeten carbonated beverages as Coke
may negatively affect bone.
Possible effects of cola extracts were also found out. Cola contains catechins, theobromine, and tannins.
Catechins, which are also found in tea, may have a positive effect on bone . However, it remains possible that other
components in cola extract could have a deleterious effect.