ROERO VALENTINA
RESANI GUIDO
Vitamina K family comprises several derivatives of 2-methyl-1,4-naphthoquinone:
- Vitamin K1 or Phylloquinone (2-methyl-3-phytyl-1,4-naphthoquinone) is synthesized by plants and constitutes the most represented form in diet;

- Vitamina K2 or menaquinones of bacterial origin (synthesized by symbiotic bacteria of the intestinal flora);

- Vitamina K3 or menadione, of synthetic origin.

Vitamin K
Vitamin K is essential for vitamin K-dependent protein carboxylation, carried out by the enzyme gamma-glutamyl carboxylase also called vitamin K-dependent carboxylase, that through the oxidation of vitamin k hydroquinone to vitamin K epoxid allows the addiction of a carboxylic acid functional group to a glutamate amino acid residue in a protein, to form a gamma-carboxyglutamate (Gla) residue, obtaining a "Gla protein".
Vitamin K-dependent carboxylation, 2008
At this time, 16 human proteins with Gla domains have been discovered, and they play key roles in the regulation of three physiological processes:
* Blood coagulation: prothrombin (factor II), factors VII, IX, and X, and proteins C, S, and Z;
* Bone metabolism: osteocalcin, also called bone Gla protein (BGP), matrix Gla protein (MGP), periostin, and the recently discovered Gla-rich protein (GRP);
* Vascular biology: growth arrest-specific protein 6 (Gas6);
* Unknown function: proline-rich g-carboxy glutamyl proteins (PRGPs) 1 and 2, and transmembrane g-carboxy glutamyl proteins (TMGs) 3 and 4.
The presence of two -COOH (carboxylate) groups on the same carbon in the gamma-carboxyglutamate residue allows Gla proteins to chelate calcium ions. The binding of calcium ion is essential to allow the activation of these proteins.
Within the cell, vitamin K epoxid (oxidized) is reduced to vitamin K hydroquinone by the enzyme vitamin K epoxide reductase (VKOR).
The reduction and subsequent reoxidation of vitamin K coupled with carboxylation of Glu is called vitamin K cycle.
The vitamin K oxidoreductase is a multimer that efficiently reduces vitamin K epoxide to hydroquinone to allow vitamin K-dependent protein carboxylation, 2013
Warfarin and other 4-hydroxycoumarins block the action of the VKOR. This results in decreased concentrations of vitamin K and vitamin K hydroquinone in the tissues, such that the carboxylation reaction catalyzed by the glutamyl carboxylase is inefficient.
http://www.rxlist.com/coumadin-drug/clinical-pharmacology.htm

Regarding the coagulation, vitamin K is important for the hepatic synthesis of coagulation factors II (prothrombin), VII, IX, X (clotting factors), and protein C with his cofactor protein S (endogenous anticoagulants).

Oral anticoagulants exert their effect by blocking the utilization of vitamin K. Systematic dose-response studies were carried out on competitive aspects of oral anticoagulants interaction with dietary vitamin K and show that dietary intakes of phylloquinone (vitamin K1) are associated to the sensitivity and stability of anticoagulation during initiation and maintenance dosing.
A study was carried on the response to weekly incremental doses (50 µg-500 µg) of vitamin K(1) supplements taken daily for 7 days. The threshold K(1) dose causing a statistically significant lowering of the INR was 150 µg/day. In 25% of the participants the INR change was regarded as clinically relevant at a vitamin K intake of 150 µg/day.
Effect of vitamin K intake on the stability of oral anticoagulant treatment: dose-response relationships in healthy subjects, 2004
High vitamin K intake can decrease the therapeutic effectiveness of warfarin. Very large amounts of vitamin K from a single meal with vegetables (400 g of vegetables with 700 to 1500 µg of vitamin K1) can measurably change INR. Warfarin requirements may change in those altering their intake of dark-green vegetables.
Influence of Vitamin K on Anticoagulant Therapy Depends on Vitamin K Status and the Source and Chemical Forms of Vitamin K, 2005
Vitamin K intake of more than 250 µg/day was shown to decrease warfarin sensitivity in anticoagulated patients consuming regular diets. Patients that were allocated to an 80% decrease of vitamin K intake increased International Normalized Ratio (INR) by almost 30% 7 days after the intervention. Similarly, it was estimated by dietary records that for each increase in 100 µg of vitamin K intake, the INR would be reduced by 0.2.
Dietary vitamin K intake and anticoagulation in elderly patients, 2007
A study was conducted on 53 patients with stably controlled anticoagulation. Each patient was asked to complete a dietary record of all foods consumed on a daily basis for 4 weeks. Each week a blood sample was taken.
Regression analysis of the data showed that, for each increase of 100 µg in the daily dietary intake of vitamin K averaged over 4 day, the INR was reduced by 0.2. This means that vitamin K has a dose dependent effect on INR in patient on Warfarin stably anticoagulated.
Dietary vitamin K influences intra-individual variability in anticoagulant response to warfarin, 2004
It was demonstrated that there is a progressive, statistically significant inverse association between the vitamin K intake score and different levels of anticoagulation, assessed by INR.
Role of dietary vitamin K intake in chronic oral anticoagulation, 2004
In chronic anticoagulated patients brief periods of changes in dietary vitamin K intake significantly alters coagulation parameters and plays a major role in INR fluctuations.
Dietary vitamin K intake and anticoagulation in elderly patients, 2007
A weekly change of 714 µg dietary vitamin K significantly altered weekly INR by 1 unit. Patients receiving warfarin therapy are instructed to maintain consistent vitamin K intakes.
Dietary vitamin K variability affects International Normalized Ratio (INR) coagulation indices, 2006
On the other hand wide evidence proves the importance of introducing a sufficiently high dose of vitamin K with diet, in order to improve anticoagulation control and thus the safety of therapy.
Poor vitamin K status appears to increase the sensitivity to small changes in vitamin K intake, especially from supplements.
Influence of vitamin K on anticoagulant therapy depends on vitamin K status and the source and chemical forms of vitamin K, 2005
The addition of 150 micrograms (µg) oral vitamin K significantly improved anticoagulation control in those with unexplained instability of response to warfarin.
Vitamin K for improved anticoagulation control in patients receiving warfarin, 2014.
Patients receiving warfarin who have unstable control of anticoagulation have a significantly lower intake of dietary vitamin K compared with their stable counterparts. Vitamin K supplementation (150 µg oral vitamin K vs placebo) resulted in a significantly greater decrease in standard deviation of international normalized ratio (INR) compared with placebo and a significantly greater increase in percentage time within target INR range. Concomitant supplementation of vitamin K, perhaps through reducing the relative day-to-day variability in dietary vitamin K intake, can significantly improve anticoagulation control in patients with unexplained instability of response to warfarin.
Vitamin K supplementation can improve stability of anticoagulation for patients with unexplained variability in response to warfarin, 2007
Compared to patients with a normal usual vitamin K intake, those with a high vitamin K intake had a decreased risk of a subtherapeutic INR. A high vitamin K intake reduces the risk of a low INR by lessening the influence of incidental consumption of vitamin K rich food on the INR.
Influence of dietary vitamin K intake on subtherapeutic oral anticoagulant therapy, 2010.
In conclusion it is widely assumed that a dietary vitamin K-warfarin interaction exists. Vitamin K can decrease the sensitivity to oral anticoagulants, nonetheless a sufficient dose of dietary vitamin K is required to stabilize the response to the OA therapy, while low and erratic intake of vitamin K can cause instability of INR. The real problem is variability in vitamin K levels, which follows erratic dietary intake. This causes variability in response to OAs and so INR instability. For this cause patients receiving warfarin therapy are instructed to maintain consistent vitamin K intakes.
A long-term oral anticoagulant therapy results in suppression of the synthesis of both vitamin K-dependent coagulation factors and Protein C, but the production of the coagulant and anticoagulant proteins is well-balanced.
Plasma levels of protein C and vitamin K-dependent coagulation factors in patients on long-term oral anticoagulant therapy, 1986
During chronic warfarin therapy the patient needs to pay attention to keep as costant as possible the intake of K vitamin because a sporadic increased intake brings to an increased balanced production of both coagulation factors and anticoagulant proteins.
However, because the half-life of protein C is lower than those of the clotting factors, it leads to a decrease in INR.

http://www.ashp.org/doclibrary/bookstore/p2548/sample-chapter-24.pdf
For the same reason we must be careful at the beginning of warfarin therapy in order to avoid a transient hypercoaguable state resultant from depletion of endogenous anticoagulants with persistent activity of endogenous clotting factors.
Warfarin, to load or not to load?
La terapia anticoagulante orale: introduzione e aspetti generali
This fact is confirmed by both the guidelines provided to doctors and the patient guides on Warfarin therapy management.
This is an extract from a guide line for doctors:
"The effect of warfarin may be inhibited by very high dietary or supplemental vitamin K intake. It is generally recommended that patients on warfarin try to consume the adequate intake for vitamin K (90-120 nicrog), while avoiding large fluctuations in vitamin K intake that might interfere with the adjustment of their anticoagulant dose."
Warfarin therapy management, 2010.
The following are the Dietary Reference Intakes (DRIs) (Recommended Dietary Allowances and Adequate Intakes, Vitamins) provided by the Food and Nutrition Board, Institute of Medicine, National Academies.
The Food and Nutrition Board at the Institute of Medicine Recommended Intakes for Individuals - Adequate Intakes (AIs) for vitamin K:
Infants
* 0 - 6 months: 2.0 micrograms per day (mcg/day)
* 7 - 12 months: 2.5 mcg/day
Children
* 1 - 3 years: 30 mcg/day
* 4 - 8 years: 55 mcg/day
* 9 - 13 years: 60 mcg/day
Adolescents and Adults
* Males and females age 14 - 18: 75 mcg/day
* Males and females age 19 and older: 90 mcg/day
http://www.nlm.nih.gov/medlineplus/ency/article/002407.htm
http://www.nal.usda.gov/fnic/DRI/DRI_Tables/RDA_AI_vitamins_elements.pdf
http://lpi.oregonstate.edu/infocenter/vitamins/vitaminK/
The following is an extract from a guide for patients:
"To help warfarin (Coumadin) work effectively, it is important to keep your vitamin K intake as consistent as possible. Sudden increases in vitamin K intake may decrease the effect of warfarin (Coumadin). On the other hand, greatly lowering your vitamin K intake could increase the effect of warfarin (Coumadin). Keep vitamin K intake constant from day to day. For example, you may plan to eat only ½ cup of foods rich in vitamin K per day. If you like these foods and eat them often, you can eat more, but be consistent. Do not make any major changes in your intake of foods rich in vitamin K. Carefully consider dietary supplements.”
http://www.bcguidelines.ca/pdf/warfarin_management_food_guide.pdf
http://www.cc.nih.gov/ccc/patient_education/drug_nutrient/coumadin1.pdf
Food Values are from the U.S. Department of Agriculture, Agricultural Research Service. USDA National Nutrient Database for Standard Reference.
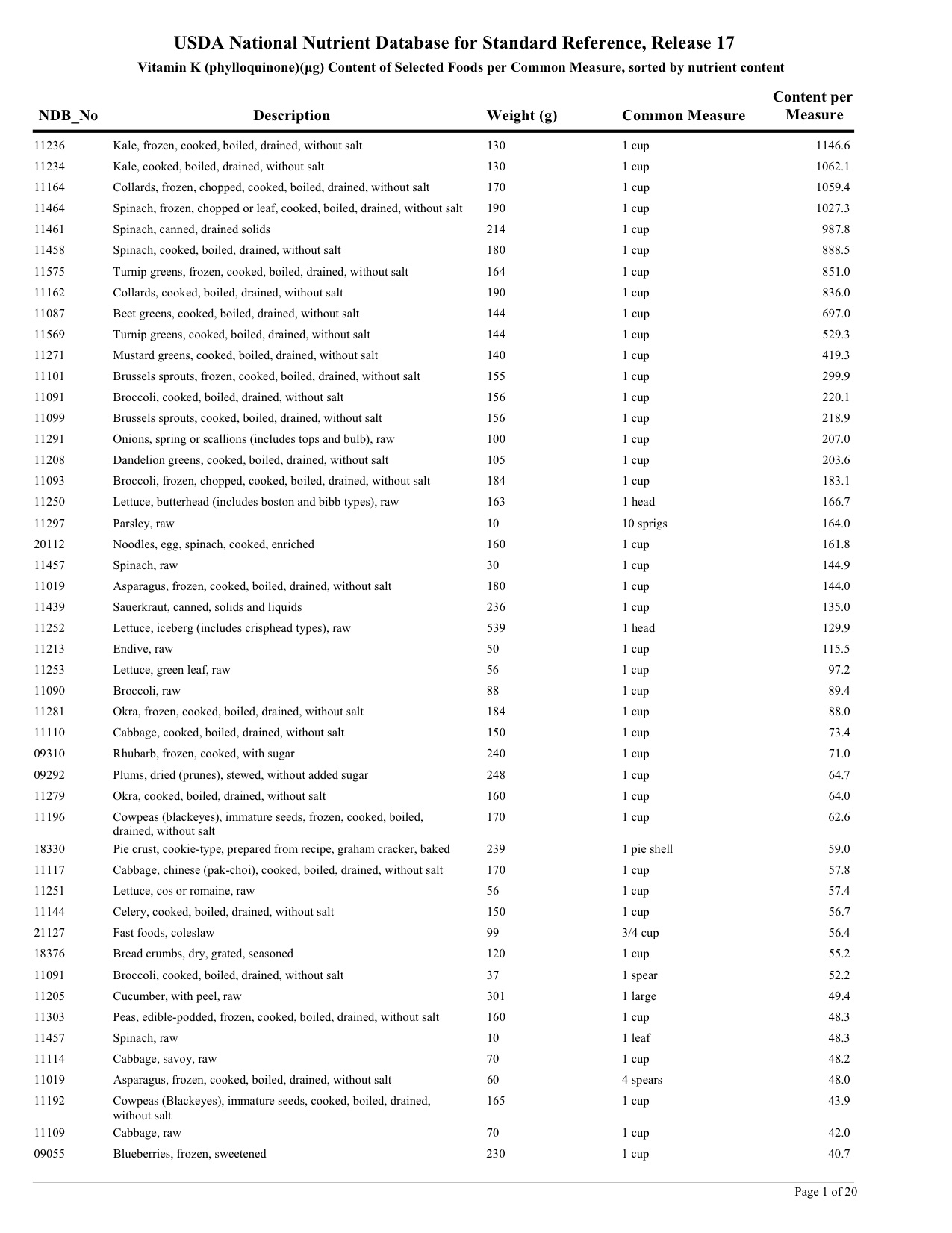
http://www.ars.usda.gov/nutrientdata