DEFINITION
The disease definition according to a specific consensus conference or to The Diseases Database based on the Unified Medical Language System (NLM)
Also the link to the corresponding Mesh term has to be created
Se ci sono più voci su OMIM usare questo formato di ricerca:
 bone marrow aplasia
bone marrow aplasia
EPIDEMIOLOGY
age, sex, seasonality, etc
SYMPTOMS
DIAGNOSIS
histopathology
radiology
NMR
laboratory tests
PATHOGENESIS
PATIENT RISK FACTORS
Vascular
Genetic
Acquired
Hormonal
Genetic
Acquired
TISSUE SPECIFIC RISK FACTORS
anatomical (due its structure)
vascular (due to the local circulation)
physiopathological (due to tissue function and activity)
COMPLICATIONS
THERAPY
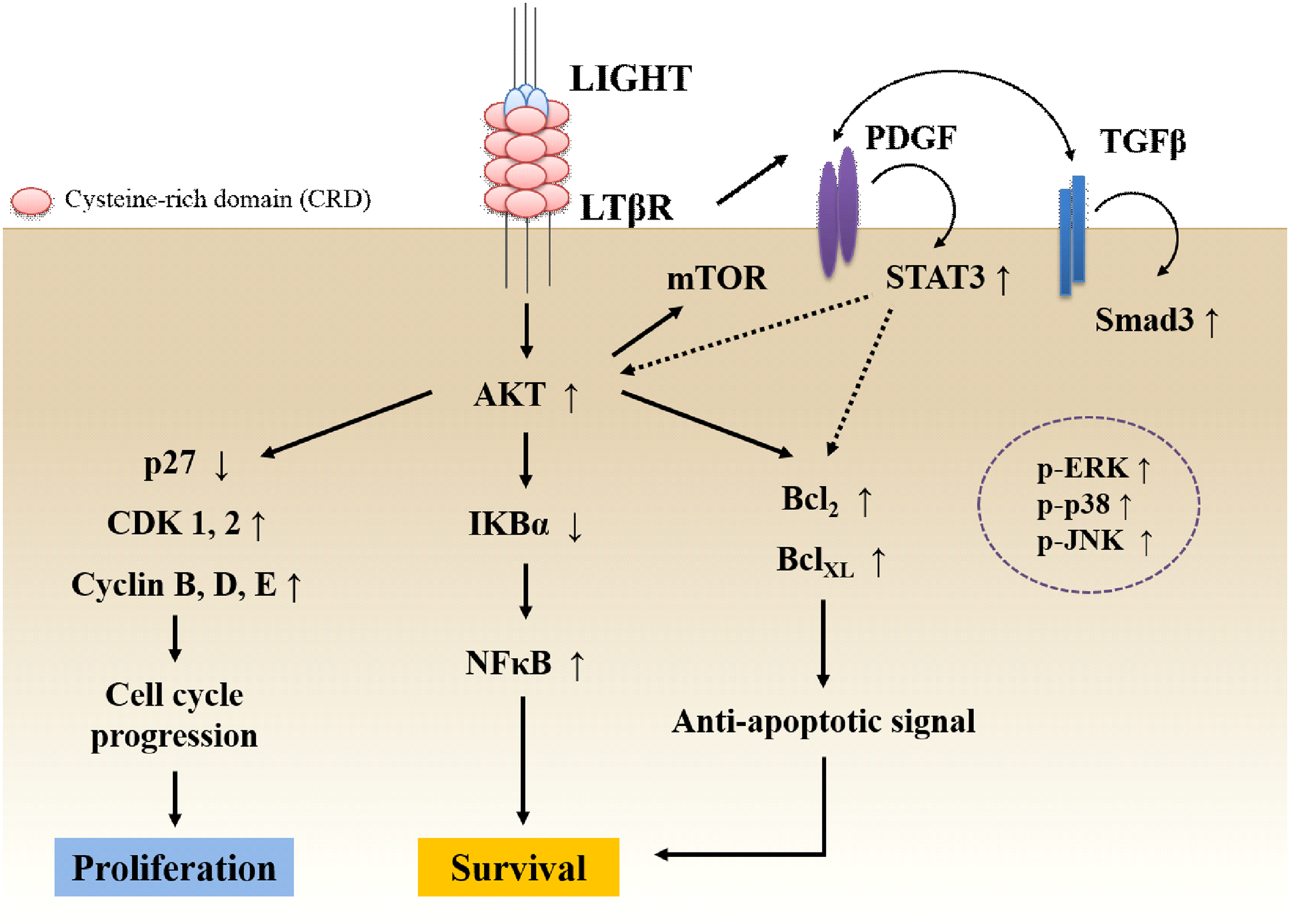
LIGHT (TNFSF14) Increases the Survival and Proliferation of Human Bone Marrow-Derived Mesenchymal Stem Cells
Ann Intern Med. 2011 Jun 21;154(12):814-23.
Assessment of thiopurine s-methyltransferase activity in patients prescribed thiopurines: a systematic review. 2011
Background: The evidence for testing thiopurine S-methyltransferase (TPMT) enzymatic activity or genotype before starting therapy with thiopurine-based drugs is unclear. Purpose: To examine the sensitivity and specificity of TPMT genotyping for TPMT enzymatic activity, reducing harm from thiopurine by pretesting, and the association of thiopurine toxicity with TPMT status in adults and children with chronic inflammatory diseases. Data Sources: MEDLINE, EMBASE, the Cochrane Library, and Ovid HealthSTAR (from inception to December 2010) and BIOSIS and Genetics Abstracts (to May 2009). Study Selection: Two reviewers screened records and identified relevant studies in English. Data Extraction: Data on patient characteristics, outcomes, and risk for bias were extracted by one reviewer and independently identified by another. Data Synthesis: 54 observational studies and 1 randomized, controlled trial were included. Insufficient evidence addressed the effectiveness of pretesting. Genotyping sensitivity to identify patients with low and intermediate TPMT enzymatic activity ranged from 70.33% to 86.15% (lower-bound 95% CI, 54.52% to 70.88%; upper-bound CI, 78.50% to 96.33%). Sparse data precluded estimation of genotype sensitivity to identify patients with low to absent enzymatic activity. Genotyping specificity approached 100%. Compared with noncarriers, heterozygous and homozygous genotypes were both associated with leukopenia (odds ratios, 4.29 [CI, 2.67 to 6.89] and 20.84 [CI, 3.42 to 126.89], respectively). Compared with intermediate or normal activity, low TPMT enzymatic activity was significantly associated with myelotoxicity and leukopenia. Limitation: Available evidence was not rigorous and was underpowered to detect a difference in outcomes. Conclusion: Insufficient evidence addresses the effectiveness of TPMT pretesting in patients with chronic inflammatory diseases. Estimates of the sensitivity of genotyping are imprecise. Evidence confirms the known associations of leukopenia or myelotoxicity with reduced TPMT activity or variant genotype. Primary Funding Source: Agency for Healthcare Research and Quality.