Iuri Unali Maurizio Lai
DESCRIPTION
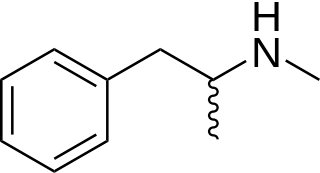
Methamphetamine is a member of the family of phenethylamines, is chiral, with two isomers, levorotatory and dextrorotatory. The levorotatory form, called levomethamphetamine, is an over-the-counter drug used in inhalers for nasal decongestion. Methamphetamine is a psychostimulant and sympathomimetic drug. It is a member of the amphetamine group of sympathomimetic amines. Methamphetamine can induce effects such as euphoria, increased alertness and energy, and enhanced self-esteem. It is a scheduled drug in most countries due to its high potential for addiction and abuse.
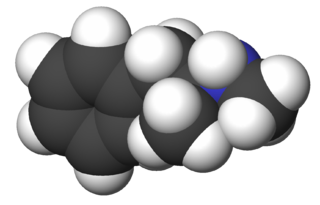
3D structure
CLASS
- Phenethylamines
- Amphetamines
- Adrenergic Agents
- Dopamine Agents
- Dopamine Uptake Inhibitors
- Adrenergic Uptake Inhibitors
- CNS Stimulants
- Sympathomimetics
| CAS number | 537-46-2 |
| Weight Average | 149.2328 |
| Monoisotopic | 149.120449485 |
| Chemical Formula | C10H15N |
| InChI Key | InChIKey=MYWUZJCMWCOHBA-VIFPVBQESA-N |
| InChI | InChI=1S/C10H15N/c1-9(11-2)8-10-6-4-3-5-7-10/h3-7,9,11H,8H2,1-2H3/t9-/m0/s1 |
| IUPAC Name | methyl[(2S)-1-phenylpropan-2-yl]amine |
| Mass Spec | (2.96 KB) |
- Substructures:
- Aliphatic and Aryl Amines
- Benzene and Derivatives
- Phenethylamines
- Aromatic compounds
- Amphetamines
INDICATIONS
Methamphetamine has occasional therapeutic use in the treatment of narcolepsy, for the treatment of Attention Deficit Disorder with Hyperactivity (ADHD) and exogenous obesity.
Methamphetamine is a potent central nervous system stimulant which affects neurochemical mechanisms responsible for regulating heart rate, body temperature, blood pressure, appetite, attention, mood and responses associated with alertness or alarm conditions. The acute effects of the drug closely resemble the physiological and psychological effects of an epinephrine-provoked fight-or-flight response, including increased heart rate and blood pressure, vasoconstriction (constriction of the arterial walls), bronchodilation, and hyperglycemia (increased blood sugar). Users experience an increase in focus, increased mental alertness, and the elimination of fatigue, as well as a decrease in appetite.
Following oral administration, methamphetamine is readily absorbed into the bloodstream, with peak plasma concentrations achieved in approximately 3.13 to 6.3 hours post ingestion. The amphetamine metabolite peaks at 10 to 24 hours. Methamphetamine is also well absorbed following inhalation and following intranasal administration. It is distributed to most parts of the body. Methamphetamine is known to produce central effects similar to the other stimulants, but at smaller doses, with fewer peripheral effects. Methamphetamine's high lipophilicity also allows it to cross the blood brain barrier faster than other stimulants, where it is more stable against degradation by monoamine oxidase (MAO).
Methamphetamine is metabolized in the liver with the main metabolites being amphetamine (active) and 4-hydroxymethamphetamine (pholedrine); other minor metabolites include 4-hydroxyamphetamine, norephedrine, and 4-hydroxynorephedrine. Other drugs metabolized to amphetamine and methamphetamine include benzphetamine, furfenorex, and famprofazone. Selegiline (marketed as Deprenyl, EMSAM, and others) is metabolized into the less active L-isomer of amphetamine and the inactive L-isomer of methamphetamine. Although only the D-Isomer of selegiline will metabolize into active metabolites, both isomers may cause a positive result for methamphetamine and amphetamine on a drug test, in certain cases. It is excreted by the kidneys, with the rate of excretion into the urine heavily influenced by urinary pH. Between 30-54% of an oral dose is excreted in urine as unchanged methamphetamine and 10-23% as unchanged amphetamine. Following an intravenous dose, 45% is excreted as unchanged parent drug and 7% amphetamine. The half-life of methamphetamine is variable with a mean value of between 9 and 12 hours.
Methamphetamine is a potent central nervous system stimulant that affects neurochemical mechanisms responsible for regulating heart rate, body temperature , blood pressure, appetite, attention, mood and emotional responses associated with alertness or alarming conditions (The clinical toxicology of metamfetamine ) . The acute physical effects of the drug closely resemble the physiological and psychological effects of an epinephrine-provoked fight-or-flight response, including increased heart rate and blood pressure, vasoconstriction (constriction of the arterial walls), bronchodilation, and hyperglycemia (increased blood sugar). Users experience an increase in focus, increased mental alertness, and the elimination of fatigue, as well as a decrease in appetite. It is known to produce central effects similar to the other stimulants, but at smaller doses, with fewer peripheral effects. Methamphetamine's fat solubility also allows it to enter the brain faster than other stimulants, where it is more stable against degradation by monoamine oxidase (MAO-A , MAO-B ) . The methyl group is responsible for the potentiation of effects as compared to the related compound amphetamine, rendering the substance more lipid-soluble, enhancing transport across the blood–brain barrier, and more stable against enzymatic degradation by monoamine oxidase (MAO). Methamphetamine causes the norepinephrine , dopamine , and serotonin (5HT) transporters to reverse their direction of flow. This inversion leads to a release of these transmitters from the vesicles to the cytoplasm and from the cytoplasm to the synapse, causing increased stimulation of post-synaptic receptors. Methamphetamine also indirectly prevents the reuptake of these neurotransmitters, causing them to remain in the synaptic cleft for a prolonged period. Methamphetamine also interacts with TAAR1 to trigger phosphorylation of PKA and PKC, ultimately resulting in the internalization of dopamine transporters. The presynaptic cell is less able to effectively remove dopamine from the synapse. The binding of methamphetamine to TAAR1 also activates adenylyl cyclase, which allows for increased intracellular cAMP. Taken together, the binding of methamphetamine to TAAR1 results in a massive efflux of neurogenic monoamines with a sustained synaptic presence. Studies have implicated methamphetamine exposure as a contributor to the development of Parkinson’s disease . High doses of methamphetamine produce losses in several markers of brain dopamine and serotonin neurons. Dopamine and serotonin concentrations, dopamine and 5HT uptake sites, and tyrosine and tryptophan hydroxylase activities are reduced after the administration of methamphetamine. Recent research published in the Journal of Pharmacology And Experimental Therapeutics indicates that methamphetamine binds to and activates a G protein-coupled receptor called TAAR1. TAARs are a newly discovered receptor family whose members are activated by a number of amphetamine-like molecules called trace amines, thyronamines, and certain volatile odorants. It has been demonstrated that a high ambient temperature increases the neurotoxic effects of methamphetamine.

Manifestations of acute overdosage with methamphetamine include restlessness, tremor, hyperreflexia, rapid respiration, confusion, assaultiveness, hallucinations, panic states, hyperpyrexia, and rhabdomyolysis. Fatigue and depression usually follow the central stimulation. Cardiovascular effects include arrhythmias, hypertension or hypotension, and circulatory collapse. Gastrointestinal symptoms include nausea, vomiting, diarrhea, and abdominal cramps. Fatal poisoning usually terminates in convulsions and coma.
Methamphetamine is highly addictive. To combat addiction, doctors are beginning to use other forms of stimulants such as dextroamphetamine, the dextrorotatory isomer of the amphetamine molecule, to break the addiction cycle in a method similar to the use of methadone in the treatment of heroin addicts. There are no publicly available drugs comparable to naloxone, which blocks opiate receptors and is therefore used in treating opiate dependence, for use with methamphetamine problems. However, experiments with some monoamine reuptake inhibitors such as indatraline have been successful in blocking the action of methamphetamine. There are studies indicating that fluoxetine, bupropion and imipramine may reduce craving and improve adherence to treatment. Research has also suggested that modafinil can help addicts quit methamphetamine use, as can Topiramate. Methamphetamine addiction is one of the most difficult forms of addictions to treat. Bupropion, aripiprazole, and baclofen have been employed to treat post - withdrawal cravings, although the success rate is low. Modafinil is somewhat more successful, but this is a Class IV scheduled drug. Ibogaine has been used with success in Europe, where it is a Class I drug and available only for scientific research. Mirtazapine has been reported useful in some small - population studies. As the phenethylamine phentermine is a constitutional isomer of methamphetamine, it has been suggested that it may be effective in treating methamphetamine addiction. Phentermine is a central nervous system stimulant that acts on dopamine and norepinephrine. Abrupt interruption of chronic methamphetamine use results in the withdrawal syndrome in almost 90% of the cases. The mental depression associated with methamphetamine withdrawal lasts longer and is more severe than that of cocaine withdrawal. Withdrawal symptoms of methamphetamine primarily consist of fatigue, depression and an increased appetite. Symptoms may last for days with occasional use and weeks or months with chronic use, with severity dependent on the length of time and the amount of methamphetamine used. Withdrawal symptoms may also include anxiety, irritability, headaches, agitation, akathisia, hypersomnia (excessive sleeping), vivid or lucid dreams, deep REM sleep and suicidal ideation.
Bibliography & Sitography
TAAR1
Methamphetamine, Drug Bank
3D Image of the molecule of Methamphetamine, Drug Bank
Amine oxidase [flavin-containing] A, Drug Bank
Amine oxidase [flavin-containing] B, Drug Bank
Solute carrier family 22 member 3, Drug Bank
Organic cation/carnitine transporter 2, Drug Bank
Sodium-dependent serotonin transporter, Drug Bank
Sodium-dependent dopamine transporter, Drug Bank
Trace amine-associated receptor 1, Drug Bank
Methamphetamine Pharmacokinetics
Methamphetamine Pathway
Methamphetamine Wikipedia
Image of the molecule of Methamphetamine, Wikimedia
3D Image of the molecule of Methamphetamine, Wikimedia
Methamphetamine Addiction
Methamphetamine, Induced Neurotoxicity
The clinical toxicology of metamfetamine
Methamphetamine Addiction