Cough is a common and protective reflex, but persistent coughing is debilitating and impairs quality of life. Antitussive treatment using opioids is limited by unacceptable side effects, and there is a great need for more effective remedies. Many studies demonstrates that theobromine, a methylxanthine derivative present in cocoa, effectively inhibits citric acid induced cough in guinea-pigs in vivo. Furthermore, in a randomized, double-blind, placebocontrolled study in man, theobromine suppresses capsaicin-induced cough with no adverse effects. The actions of theobromine appear to be peripherally mediated. We conclude theobromine is a novel and promising treatment, which may form the basis for a new class of antitussive drugs.
Cough
Cough helps us to remove inhaled foreign bodies and excessive ecretions from the respiratory tract. The main anatomical areas stimulating the cough reflex are located in the upper airways, in particular the larynx.
The cough reflex is initiated by stimulation of two different classes of sensory afferent fiber, namely the myelinated rapidly adapting receptors (RAR) and nonmyelinated C-fibers with bronchial or pulmonary endings (vagal fibers). Inappropriate activation of these nerves lead to many of the symptoms such as coughing. However, the mechanisms involved in the abnormal functioning of airway nerves have not yet been described. They are thought to involve the release of inflammatory mediators which sensitize the nerve fibers; this leads to an increased electrical activity of these fibers wich will release various neurotransmitters from the nerve endings. We hypothesize that agents that inhibit sensory nerve activity will also inhibit the cough reflex.
Narcotic agents with a morphine skeleton, such as the opioids codeine and dextromethorphan, are the most used antitussives in cough remedies, but they have unpredictable efficacy and undesirable central nervous and peripheral side effects. For these reasons there is the need to find an alternative treatment.
Usmani O. S.,Theobromine inhibits sensory nerve activation and cough,2004
Morice A. H.,Cough,2002
Opioid antitussives
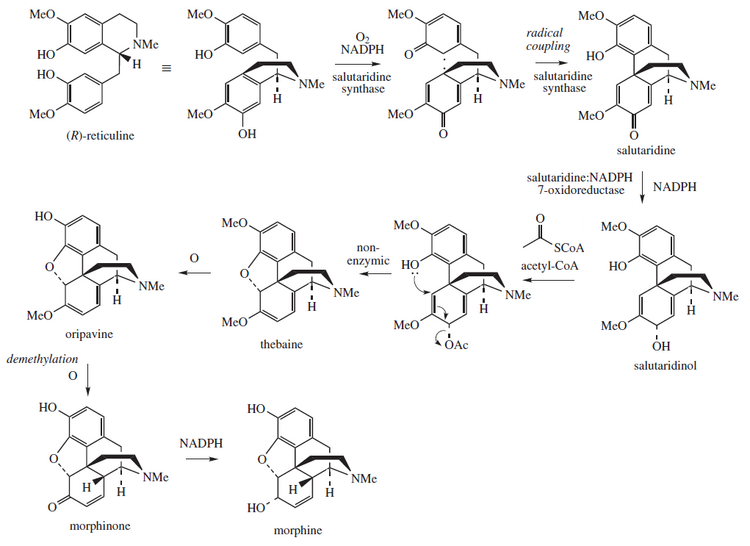
The original opiates, morphine and codeine, are derived from opium. Over the years, thousands of derivatives were synthesized to try to dissociate analgesia from side effects, particularly respiratory depression, constipation, and dependence liability.
De Blasio F.,Cough management: a pratical approach,2011
Opioid receptors
Opioids produce effects on neurons by acting on receptors located on neuronal cell membranes. There are three main types of opioid receptors: µ, δ, κ. These receptors belong to the large family of receptors which possess 7 transmembrane-spanning domains of amino acids.
Pharmacological studies have shown that the naturally occurring opioid peptide, β endorphin, interacts preferentially with µ receptors, the enkephalins with δ receptors and dynorphin with κ receptors. Morphine has considerably higher affinity for µ receptors than for other opioid receptors. All three receptors produce analgesia when an opioid binds to them. However, activation of κ receptors does not produce as much physical dependence as activation of µ receptors.
The opioid receptors and many other membrane receptors are coupled to guanine nucleotide binding proteins known as G-proteins. G-proteins consist of 3 subunits (α, β and γ). When the receptor is occupied, the α subunit is uncoupled and forms a complex which interacts with cellular systems to produce an effect.
Several types of G-proteins have been found. The types to which the opioid receptors are coupled produce inhibitory effects in neurons.

Opioid inhibition of neurotransmitter release
Neurotransmitter release from neurons is normally preceded by depolarisation of the nerve terminal and Ca++ entry through voltage-sensitive Ca++ channels. Drugs may inhibit neurotransmitter release by a direct effect on Ca++ channels to reduce Ca ++ entry, or indirectly by increasing the outward K + current (increased outward movement of K+ is the most likely mechanism for the postsynaptic hyperpolarisation and inhibition of neurons induced by opioids throughout the nervous system), thus shortening repolarisation time and the duration of the action potential. Opioids produce both of these effects because opioid receptors are apparently coupled via G-proteins directly to K+ channels and voltage-sensitive Ca++ channels . Opioids also interact with other intracellular effector mechanisms, the most important being the adenylate cyclase system.

Chahl L.,Opioids:mechanisms of action,1996
Side effects of codeine
The most frequent side effects of codeine include lightheadedness, dizziness, nausea, vomiting, shortness of breath and sedation. Other side effects include allergic reactions, constipation, abnormal pain, rash and itching.
Mental and physical dependence can occur but are unlikely when used for short-term pain relief. If codeine is suddenly withdrawn after prolonged use, symptoms of withdrawal may develop. The dose of codeine should be reduced gradually in order to avoid withdrawal symptoms.
Analgesic Tolerance
The prolongued opioid use leads to a progressive decline in potency, a phenomenon termed ‘tolerance’; so the dose of opioids must be increased to maintain a fixed response. Tolerance is due to a wide variety of responses, ranging from biochemical changes at the receptor to more generalized changes within N-methyl-D-aspartate (NMDA) neuronal circuits.
video
Opioid dependence
Dependence is a physiological response to chronic administration of opioids. It has been most
closely studied with µ opioids. It is important to distinguish dependence from addiction. Dependence is a physiological response seen in all subjects maintained on opioids, whereas addiction implies a psychological dependence and is uncommonly seen in patients with no prior history of drug abuse. Clinically, dependence is not a concern as long as patients continue to take their opioid. Antagonists can precipitate withdrawal within seconds. However, with care it is possible to reverse opioid actions without precipitating withdrawal by diluting the antagonist and slowly titrating it against the patient’s signs and symptoms.
Other actions
Morphine and related drugs have a variety of other actions in addition to analgesia, including respiratory depression and the inhibition of gastrointestinal transit, which plays a major role in the constipation seen in most patients. Opioids also have a number of neuroendocrine actions, influencing the secretion of prolactin, growth hormone, testosterone, and a variety of other hormones. Although both actions are mediated through µ receptors.
Mellar P. Davis,Opioids in cancer pain,2009
Theobromine
Theobromine belongs to a class of alkaloid molecules known as methylxanthines. Methylxanthines naturally occur in as many as sixty different plant species and include caffeine (the primary methlyxanthine in coffee) and theophylline (the primary methylxanthine in tea). Theobromine is the primary methylxanthine found in products of the cocoa tree, theobroma cacao.
Different types of chocolate contain different amounts of theobromine. In general, theobromine levels are higher in dark chocolates (approximately 10 g/kg) than in milk chocolates (1-5 g/kg). Higher quality chocolate tends to contain more theobromine than lower quality chocolate. Cocoa beans naturally contain approximately 300-1200 mg/ounce theobromine.

"Fredholm B.,Methylxanthines,2004"
Theobromine absorption from the digestive tract is slow, especially compared with caffeine, with an estimated peak plasma time of 2.5 h.
In humans, methylxanthines are metabolised by demethylation (removal of methyl side groups) by the enzyme cytochrome P450 (CYP).Then, theobromine (3,7-dimethylxanthine) is broken down to 3-methylxanthine and 7-methylxanthine by CYP.

Mechanisms of action of theobromine
The beneficial effect of theobromine on airways is the suppressive action on cough reflex through the suppression of vagus nerve activity.
This effect was shown through a study on guinea pigs and humans; this study investigates the action of theobromine in the guinea pig cough model in vivo, and in isolated human and guinea-pig vagus nerve preparations in vitro.
It was observed that theobromine inhibit cough in human trial at concentrations that do not have central side effects in man. Cough was induced by citric acid aerosol on guinea pigs and by capsaicin aerosol on humans, and comparing the drug-treated groups with the control groups, a statistical significance was taken a P < 0.05.
The results demonstrate that theobromine and codeine show a dose-dependent antitussive effect on citric acid-induced cough in guinea pigs compared with the vehicle-treated control groups, but theobromine at a dose of 32 mg/kg produce a long-lasting antitussive effect.
In human study, no adverse effects were observed of the cardiovascular or central nervous
(on the contrary of codeine), and these data support the use of theobromine as an effective antitussive agent in man, with a safe therapeutic index.
Usmani O. S., Theobromine inhibits sensory nerve activation and cough,2004
In these years some pharmaceutical companies are trying to develop new drugs based on the benevolent use of theobromine for the threatment of cough.
The basic idea behind these researches is the clinical trial conducted by Alyn Morice, Director of the Cough Clinic of the University of Hull in the United Kingdom.
Study of the Safety and Effectiveness of BC1036 Capsules to Treat Frequent Long-Term Cough
Scheske M., Healthcare established to launch novel consumer medicines,2004