
DEFINITION
The female athlete triad is an interrelationship of menstrual disfunction, low energy availability and decreased bone mass density (BMD).It is relatively common among young women participating in sports.
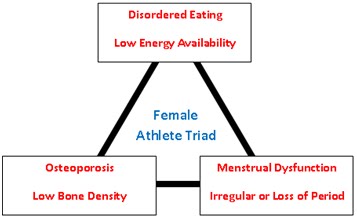
The first definition of the female athlete triad was provided by the American College of Sports and medicine; at first the triad was recognized as three separated but interrelated entities: eating/low energy availability, menstrual disturbance/amenorrhea and bone loss/osteoporosis. The female that are at risk for developing the female athlete triad are those that required to have frequent weigh-ins, consequence for weight gain in sport, pressure to win at all costs and societal pressure to look in a particular way.
The female athlete triad most commonly presents in sport that have subjective scoring on female's performance, endurance sports, sports that emphasize low body weight, sports that require the athlete to wear revealling or tight clothes.
The updated 2007 American College of Sports position stand now recognizes that the female athlete triad is a spectrum of symptoms and conditions ranging between health and disease. The three spectrum include energy availability, menstrual dysfunction and bone mineral density.
The female athlete triad, 2012
The female athlete triad: a case series and a narrative overview,2013
EPIDEMIOLOGY
Only a small percentage of athletes ( 0%-15.9% ) exhibit all of the 3 conditions currently; the prevalence of 2 components of the triad ranged from 5.4% and 26.6%
If we analyze the percentage of each condition separately we can see a difference between general population and athletic community:
- Menstrual dysfunction: the prevalence of primary and secondary amenorrhea ranged from 0%-56% and 1-60%. The prevalence in average population is 2.6%.
- Disordered of eating, such as anorexia nervosa and bulimia nervosa: the prevalence of clinical eating disorders range from 16% to 47%. The prevalence in average population is 0.5% and 10%.
- low BMD: the prevalence of osteopenia ranges from 22% to 50%, with the osteoporosis spanning 0%-13%. The prevalence in average population is 12% and 2.3% respectively.
THE COMPONENTS OF THE TRIAD
1.Menstrual dysfunction
Menstrual function range from eumenorrhea (normal menstration) to amenorrhea (no menstruation for more than 3 months). To maintain eumenorrhea female need to consume approximately 45kcal/kg free fat mass (FEM) per day. Oligomenorrhea is decribed as menstrual cycle lasting > 35 days in duration and can occur to female consuming less than 30kcal/kg FEM. Amenorrhea is describing as menstrual cycling lasting more than 90 days.
Amenorrhea can be primary or secondary.

Primary amenhorrea refers to delay in the age of menarche (no menses by age of 15 in the presence of normal normal secondary sexual development).
Secondary amenorrhea is the loss of menses after menarche. Amenorrhea can be caused both by anatomical and endocrinal disfunction.
The type of amenorrhea resulting from changes in energy availability is functional hypotalamic amenorrhea (FHA).
It is the most common type of amenorrhea in female athletes.
FHA is characterized by the the absence of menses due to the soppression of the hypotalamic-pituary-ovarian-axis, without an indentificable anatomical cause.
Physiological and neuroendocrine changes within the body will signal to the hypotalamous to stop producing gonadotropin release hormone (GnRH).
A decrease in GnRH halts the release of Luteizing hormone (LH) and follicle stimulating hormone from the pituary gland. Further, an overall decrease in LH e FSH, suppresses the ovaries from producing estrogen and progesterone leading to abnormal menses in the female athlete.
FHA can be also associated by overactivity of the hypotalamic-pituary-adrenal axis (causing an increase in cortisol release, which decreases the release of GnRh) and disturbance of the hypotalamic-thyroid axis (resulting in a sick euthyroid pattern). Even leptin, a citokyne expressed by adipose tissue and strongly associated with fat mass, is low in female athlete; leptine has positive effect on GnRH secretion and regulates the release of gonadotropins.
The female athlete triad, 2012
The female athelete triad: a case series and narrative overview.2013
2.Low energy availability
Energy avalability is the amount of dietary energy for all physiologic and function after accounting for energy expenditure from exercise.
Low energy availability may be the result of an eating disorder but can also occur in the absence of a psychiatric diagnosis.
Athletes may have disordered eating simply by unknowingly failing to attain their energy requirements secondary to time constraints or lack of nutritional knowledge.
There is a wide spectrum of disordered eating among athletes that ranges from simple dieting to clinically defined eating disorder such as anorexia nervosa, bulimina nervosa and eating disorder not otherwise specified.
Anorexia athletica is a term used by some researchers to describe a disordered eating pattern seen in the female athlete who has an intense fear of gaining weight, even though she is underweight.
Recent evidence from study of exercising women with FHA highlights the potential role of appetite-related hormones in the etiology of chronic energy deficency and menstrual disturbance.
The main appetite related hormones are:

- Ghrelin: it is mainly produced by the stomach, but it is also expressed in many other tissues. It increases food intake by the activation of the food intake signalling cascade by NPY neurons in the arcuate hypotalamous nucleus and stimulates the GH's secretion.
Ghrelin is increased in case of anorexia nervosa and this increase in plasma ghrelin levels may occur either as an adaptative response to correct the abnormal energy statutus or as a result of relative resistance to ghrelin.
In patients with anorexia nervosa the GH response to ghrelin administration is blunted.
- Obestatin: its effect on food intake and its level in anorexia nervosa are similar to the ghrelin's one.
- NPY: is the strongest orexigenic factor. It is secreted by SNS neurons. Its role can be considered as helping to coordinate protective anti-starvation activity and preventing further depletion of existing energy stores.
- PYY: is a 36-amino acid anorexigenic gut peptide belonging secreted by the endocrine L cell of the distal ileum and colon in response to feeding. Its role is to reduce caloric intake
CCK: is a gut-brain hormone secreted by the gastrointestinal system in response to food intake as well as by specialized neurons in the myenteric plexus and the brain. Its levels are high in patients with eating disorders.
- Leptin: is an anorexigenic hormone secreted by adipocytes. It suppresses appetite and regulates energy expenditure and it suppresses antivity of NPY neurons. In patients with eatinh disorders plasma leptin level is low.
As we said before appetite-related hormones have an essential role in developing low energy availability.
Elevated levels of ghrelin and PPY can be the cause of the lack of initiative to match energy intake to exercise energy expenditure; they also have a suppressive effect on appetite.
Update on the female triad, 2013
The Role of Mixed Orexigenic and Anorexigenic Signals and Autoantibodies Reacting with Appetite-Regulating Neuropeptides and Peptides of the Adipose Tissue-Gut-Brain Axis: Relevance to Food Intake and Nutritional Status in Patients with Anorexia Nervosa and Bulimia Nervosa, 2013
3.Low bone density

Generally healthy women achieve 92% of their total body bone mineral content by 18 years of age and approximately 99% by age 26 years.
Bone loss usually occurs later with menopause and aging; in young female athletes with the triad a compromise in bone strenght including the bone mineral density may occur at a much younger age. Several different components contribute to bone strenght, including bone mineral content, BMD, bone microarchitecture and bone remodelling.
A failure to accumulate sufficient bone mass during adolescent years can lead to osteoporosis, a skeletal disorders characterized by a compromised in bone strenght predisposing a persons to an increasd rick of frcture.
Various modifiable factors enhanche bone accrual : growth hormone, insulin gonadal steroids, leptin, T3, cortisol, catecholamines, paratyroid hormone.
These hormone affect skeletal growth, bone remodelling and mineralizationby direct and indirect actions on bone.
- GH : stimulates prechondrocyte proliferation in the growth plate, enhances pre-osteoblast proliferation and osteoblast differentiation and induces local and systemin production of IGF-1. In addition, exogenous administration of GH suppresses production of IGFBP-4 (which opposes the anabolic effects of IGF-I on bone) and stimulates production of IGFBP-2, -3, and -5 (which stimulate bone cells directly and/or through IGF-I).
- IGF-I : affects chondrocyte and osteoblast differentiation and action, and also enhances renal conversion of 25(OH) vitamin D to the active hormone 1,25(OH)2 vitamin D, increasing calcium and phosphorus absorption in the gut. In addition, IGF-I increases renal tubular reabsorption of phosphorus.
- Sex steroids, T4, and glucocorticoids impact the secretion of GH and IGF-I, but also have other effects on skeletal development.
- Glucocorticoids inhibit calcium absorption through a vitamin D independent mechanism and inhibit osteoblast action and survival through potentially an osteoclast mediated mechanism.
- Thyroid hormones increase bone turnover by increasing osteoblastic and osteoclastic activity.
Even many of the hormones that signal energy avalability appear to have impact on bone mass:
- leptine : stimulates efferent neuronal signalling fron the hypotalamous to receptors on osteoblast , thereby rechilating cancellous bone formation. It also has beneficial effects on cortical bone
- ghrelin : stimulation of osteoblastic activity
- PYY : deleterious effect on the bone
- cortisol : deleterious effect on bone
In addition nutritional contributions such as overall caloric consumption and calcium and vitamin D intake are crucial to mantaining an appropriate energy balance.
Young female athletes show not only a low BM, but also a lower trabecular number and higher trabecular separation. They also have a greater abundance of yellow marrow, suggesting preferential differentation of mesechymal stem cell pool into premature adipocytes rather than osteoblasts.
The female athlete triad, 2012
Bone health and the female athlete triad in adolescent athletes,2011
SCREENING AND DIAGNOSIS
The greatest challenge in treating female athletes with the triad may be making the initial diagnosis of the conditions. It is important to screen any athletes who presents with 1 one the 3 compomennts of the triad.

1.Menstrual dysfunction
To asses the menstrual status can be helpful questions about family history and maternal age of menarche. When evaluating primary or secondary amenorrhea, ethiologies such as thyroid disorders,polycystic ovarian syndrome, intrauterine devices and medications should be considered. Beacause hypotalamic amenorrhea is a diagnosis of exlusion, other ethiologies such as polycistic ovarian, adrogen secreting, thumor, hyperandrogenism must be ruled out. In athlete presenting amenorrhea laboratory testing should include:
- complete blood count and chemistry panel to rule out chronic illness associated with amenorrhea
- beta-himan gonadotropin testing to rule out pregnacy
- thyroid stimulating hormone and free thyroxine to tests primary thyroid disfunction
- prolactin to asses for pituary mass
- FSH to rule out ovarian insufficiency
- LH, in case of hyperandrogenism
- total testosterone and sex hormone blinding proteine
- total testosterone dehydroepiandrosterone
The female athlete triad, 2012
Update on the female athlete triad, 2013
2.Energy availability/disordered of eating
At first questions about eating behviors, diet, eating habits and energy expenditure can be helpful to determine energy balance in young athletes.
On the physical examination signs associated with eating disorders and low weight are:
- bradycardia
- orthostatic hypotension
- hypothermia
- Russel sign (physical signs of persistent vomiting): genigival abrasoin, parotid enlargement, loss of dental enamel
- dry skin
- hypercarotenemia
- lanugo
- acrocyanosis
To evalueted subclinical disordered of eating also a EDE-Q, Eating Disordered Inventory (EDI) and Three Factor Eating Questionnaire are useful.
Update on the female athlete triad, 2013
3.Low Bone Mass
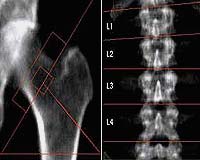
There are several imaging modalities for analysis of bone structure:
- dual energy x-ray absorptiometry : it can measure bone mass and areal BMD for the whol body as well as specific regions such as lumbar spine, hip, and distal radius. Measurement of the spine and whole body is preferred in adolescents because of the lack of precision in the hip region in identifying anatomic landmarks
- high resolution peripheral quantitative computed tomography to measure bone geometry and microstructure

COMPLICATIONS OF THE TRIAD
The complications of the triad are:
- elevated risk of fracture
- endothelial disfuction and developmentof cardiovascolar disease
Female athletes with the triad present a decrease in flow-mediated dilatation and in reactive hyperemic response due to the low concentrations of estrogens.
Estrogen has receptor on vassels and stimulates the production of nitric oxyde synthease, leading to increased the production of endothelial-derive nitric oxide ultimately leading to vasodilatation. The are many clinical implications due to reduced flow mediated dilation such as reduction in exercise capacity and performance by restricting the amount of blood to critical muscles involved in exercise and premature development of arteoschelosis.

Update on the female athlete triad, 2013
Association between the female athlete triad and the endothelial dysfuction in dancers, 2011
TREATMENT
There is still much debate on the best method of treatment for young female athletes with the Triad.
A multisciplinary team including coach, phisioterapist, sport dieticians, psychologyst is needed.
The primary focus of treatment of the triad is the modification of diet and exercise behaviors to increase energy availability subsequent resumption of menses and ideally improvement of bone metabolism.
The pharmacological therapy if often considered to help restore menstruation and provided adequate hormonal supplemntation. It includes:
- oral contraceptive pill: contains estrogen and progestin. It can be helpful to restore menstruation but its effect on BMD are controversial. A side effect of using OCP can be that it can give a false sense of improvement to young woman by restoration of menses without any change in energy availability
- transdermal estrogen: its positive effect is due to the no soppression of IGF-1, a bone trophic hormone. While oral estrogen decrase systemic IGF-1, transdermal estrogen maintains or increases IGF-1
- metreleptin (methionyl human leptin): it is helpful to restore menses and improve BMD, but it has as side effect weight-loss
- vitamina D and calcium , to restore bone health
- bisphoshonates: are used especially in postmenopausal women bacause inhibit the osteoclast function. They are not used in adolescent women beacause they remain active in bones for many years and they have potential teratrogenic effect in pregnancy
- folic acid: it is used as a treatment for decreased flow mediated dilatation because it is hypotesized to partecipate in the endogenous regeneration of tetrahydrobiopterina, an essential cofactor in the production of endotelial nitric oxide synthease
The female athlete triad, 2012
Update on the female athlete triad, 2013