Alpha-fetoprotein, a multiple indicator
AFP: an introduction
AFP is a serum glycoprotein synthesized mainly in fetal yolk sac endoderm and liver but also in a minimum fraction in the intestinal epithelium of the embryo. It binds to copper, nickel, fatty acids and bilirubin.
A gene encoding AFP is found in many species, which confirms the importance of the protein during normal development.
Human AFP is the result of the transcription of AFP gene which is located on the q arm of chromosome 4 . (4q25) Biomedichal studies have reported the presence of many genetic variants of AFP gene, differing in kilobases lenght.
Mammalian AFP is classified as part of the albuminoid gene superfamily including albumin, AFP, vitamin D (Gc) protein, and alpha-albumin. All of the four albumin genes are located in tandem on chromosome 4 in the 4q11-q22 region and present similarities in gene sequence and patterns of cysteine disulfide bridges.
Both mRNA of AFP and Albumin have been found in the liver during late fetal life, whereas only AFP mRNA is present in the yolk sac.
Alpha-fetorotein MedlinePLus
Alpha-fetoprotein
Alfafetoproteina
Alpha-fetoprotein, stem cells and cancer
Marcatori tumorali
Mapping of AFP
Structure
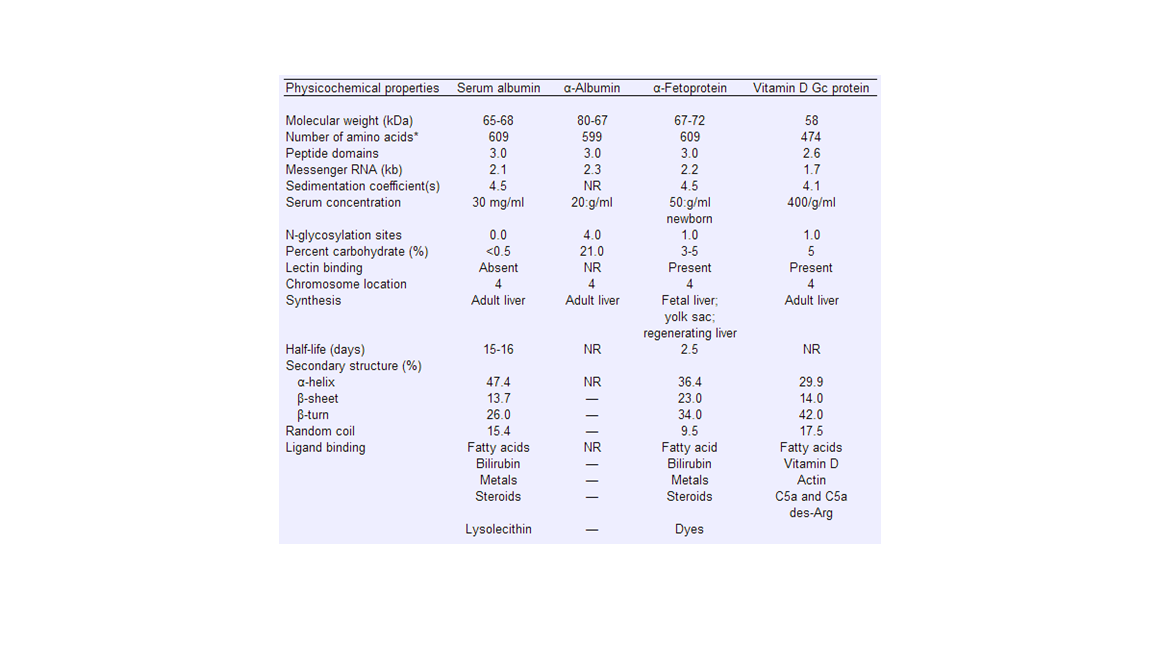
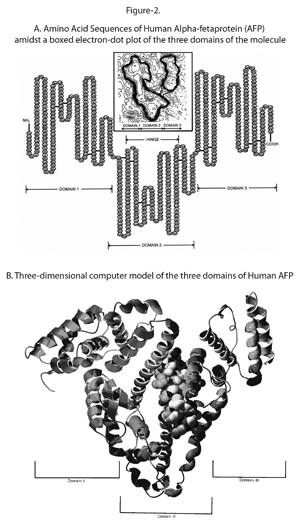
Human AFP is a single chain glycoprotein of 591 amminoacids and a carbohydrate moiety (of 5% circa). The molecular mass of 69 kDa varies depending on its carbohydrate content. Thirty-two cystein residues in the amminoacid sequence creating multiple disulfide bridges result in a V-shaped molecular structure composed of three domain. AFP can also be found in monomeric, dimeric and trimeric forms.
Alpha-fetoprotein, structure and function
Function: AFP in normal development

figure 3: AFP concentration in normal development, after liver injury, during growth of transplantable hepatoma (Morris hepatoma 7777) and during chemical hepatocarcinogenesis in mice
During development AFP levels in fetal serum and amniotic fluid increase until 12 week and remain elevated after birth for 3-4 weeks in the newborn. Since found in fetal serum part of AFP reaches maternal blood through the placenta resulting in an encrease of serum AFP level of the mother during pregnancy. Maternal serum levels rise until circa 32 weeks. However, as shown in the figure AFP level is two logs higher in fetal serum at term than in mother.
While fetal AFP level remain high after birth, serum AFP level in the mother drops exponentially.
Multiple hypoteses of AFP function have been postulated and tested though, none has revealed to be true in human. Therefore, AFP role remains unclear.
The three major functions, examined and not proven to be true in human, were:
# AFP as an immunosoppressive protein suppressing the maternal immune rejection of the fetus
# AFP as a fatty acid carrier protein partecipating in myelination brain neurons
# AFP as a estrogen receptor protecting the development of female brain from masculinization
This latter function has proven to be true in mice but of no relevance in human because human AFP doesn't bind estrogen. Although counter-intuitive, virilization of femal mouse brains occurs when a high dose of estrogens reaches the brain during development. Thus, adult female AFP knockout mice are infertile and inable to produce gonadotropins.
Values
Values of maternal serum AFP (MSAFP) level during fetal development differs in the first and second trimester
First Trimester
200 - 400 mg/dL
Second Trimester
14 weeks of gestation: 25.6 ng/mL
15 weeks of gestation: 29.9 ng/mL
16 weeks of gestation: 34.8 ng/mL
17 weeks of gestation: 40.6 ng/mL
18 weeks of gestation: 47.3 ng/mL
19 weeks of gestation: 55.1 ng/mL
20 weeks of gestation: 64.3ng/mL
21 weeks of gestation: 74.9 ng/mL
Studies report that maternal AFP level is 200% higher in case of a twin pregnancy.
Two tests of MSAFP are currently performed: a non-invasive one, where AFP is measured by taking mother’s blood during the 2nd trimester, and another one where AFP is measured from the amniotic fluid.
Since MSAFP concentration is related to AFP fetal levels, MSAFP screening is important to detect possible fetal anomalies.
MSAFP are often expressed in terms of MoM (multiple of the median).
A MoM tells how the patient result deviates from the median of the population.
multiple of the median
The normal range of MAFP values is from 0.5 to 2.0 or 2.5 MoM.
MSAFP above normal is typical of:
*neural tube defects
*spina bifida
*anencephaly
*abdominal wall defects
MSAFP below normal is specific of
*Down syndrome
*Trysomy 18
AFP has no function in adults thus, normal values in men and women (not pregnant) are below 6.0 ng/ml.
AFP concentration above this range is associated with a variety of pathology:
- Testicular cancer
- Colon cancer
- Liver cancer
- Pancreatic cancer
- Lung cancer
- Kidney cancer
- Breast cancer
- Stomach cancer
- acute hepatitis
- hepatic cirrhosis
This is how to prapare the test for AFP.
AFP test
Maternal Serum alpha-fetoprotein
Valori normali AFP
Elevated AFP
AFP production in liver injury and HCC (hepatocellular carcinoma)
AFP is produced by all lineage of liver cells during proliferation which occurs both after liver injury and during growth of hepatocellular carcinoma.
The production of AFP _appears to be the re-expression of a developmental protein. A possible explanation of this fact could be that liver cells are not terminally differentiated but, indeed, unipotent stem-cells and as such they can be activated to proliferate and self-renew. When undergoing mitosis and thus manifesting their stem-like ability, liver cells re-express a marker of liver progenitors, AFP. This ability to re-enter in the cellular cycle from Go when needed makes, also, liver cells, according to Bizzozero classification, stable cells.
A stem cells undergoes an asimmetric division creating a cell identical to the original stem cell and another cell which starts a differentiation path becoming a transit amplifyng cell. The latter divides a specified numer of time and then terminally differentiate losing the ability of entering in G1.
Stable Cells
Differenziazione cellulare
Transit amplifying cell
As shown in figure 3:
- After liver injury there is a rapid but transient elevation of serum levels both in two-thirds partial hepatectomy (PH), where the serum level in older rats is lower than in that of theyounger one, and in chemical injury (here caused by carbon tetrachloride(CCl4) and Galactosamine).
Serum levels are also lower after PH than after chemical injury.
During growth of *HCC , induced by the transplant of Morris hepatoma 7777(see above in the description of the figure) into the thigh of histocompatible rats, AFP encreases in an almost logarithmic way and decreases in the same manner after surgical removal.
*A stable elevation is seen after treatment ih a non carcenogenic dose of the carcinogen N-2acetylaminofluorene (AAF), an aromatic amine.
AAF
Liver Injury
In response to the loss of cells due to partial hepatectomy or chemical injury all liver cells
: hepatocytes and biliary cells cooperate to restore lost tissue by proliferation and produce, undergoing mitosis, AFP. Although, when a sever injury occurs or normal proliferation of hepatocytes is blocked , liver-regeneration is made by bipotential progentor cells, oval cells. Oval cells,which are found in canals of Hering (CoH), are capable of generate both hepatocytes and cholangiocytes.
All of these kinds of cells: stem cells, mature hepatocytes and ductal cells when proliferating produce AFP.
Liver rigeneration
Cellule progenitrici epatiche
Cellula staminale][http://www.content.elearning-unicam.it/repository/patologiaGenerale/modulo_4/unit_3/text.html
Rigenerazione tissutale
Cellule Staminali pluripotenti fegato
Hepatocellular carcinoma
Hepatocellular carcinoma is a common neoplasy, the eight in the world. It frequently develops from a pre-existing hepatic desease such as cirrhosis or viral hepatitis.
It can arise from stem cells, transit amplifying cells and mature hepatocytes.
All of them expressing AFP while proliferating and all of them not terminally differentiated and arrested in maturation.
Since expressed in HCC, AFP has a role as tumoral marker. However, for its low sensitivity AFP levels are not used as screening tests but are very useful to monitorate the development of HCC tumor and its response to therapy. FETO-TECT is the test kit to measure human AFP.
Serum AFP levels are higher in a tumor which is faster growing , poor differentiated and has aneuploidy.
Tumor markers in hepatocellular carcinoma
Conclusion
In conclusion, screening for AFP has two major applications: in pregnant women is used as a routine test to detect fetus anomalies, whereas in adults is used as a tumor marker for multiple types of cancer. In fact, a level above 500 nanograms/milliliter of AFP in adults can be a sign of hepatocellular carcinoma, germ cell tumors, and metastatic cancers of the liver.
Moreover, AFP as stem-cell marker is also an interesting protein confirming the unipotent stem cell nature of liver cells.
Liver cells re-express a stem-cell marker when manifesting their stem-like ability.