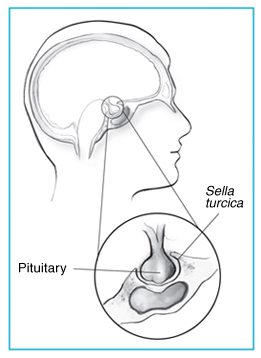
Prolactin-Secreting Pituitary Adenoma is a benign tumor (adenoma) of the pituitary gland that produces a hormone called prolactin. It is the most common type of functioning pituitary tumor. Symptoms of prolactinoma are too much prolactin in the blood (hyperprolactinemia), or those caused by pressure of the tumor on surrounding tissues.
Prolactin stimulates the breast to produce milk, and has many other functions such as regulation of mood. Hence prolactin levels are usually higher during pregnancy and after childbirth. After delivery of a baby, a mother's prolactin levels come down to normal a few weeks after breastfeeding is discontinued. Each time the milk is dispensed, prolactin levels rise; this process may cycle to maintain milk production. In males it is responsible for the sexual refractory period after orgasm (endorphins) and excess levels can lead to erectile dysfunction.
ALK7 expression in prolactinoma is associated with reduced prolactin and increased proliferation. 2018 (What role has ALK ?)
- Abstract
Prolactinoma represents the most frequent hormone-secreting pituitary tumours. These tumours appear in a benign form, but some of them can reach an invasive and aggressive stage through an unknown mechanism. Discovering markers to identify prolactinoma proliferative and invading character is therefore crucial to develop new diagnostic/prognostic strategies. Interestingly, members of the TGFβ-Activin/BMP signalling pathways have emerged as important actors of pituitary development and adult function, but their role in prolactinomas remains to be precisely determined. Here, using a heterotopic allograft model derived from a rat prolactinoma, we report that the Activins orphan type I receptor ALK7 is ectopically expressed in prolactinomas-cells. Through immunohistological approaches, we further confirm that normal prolactin-producing cells lack ALK7-expression. Using a series of human tumour samples, we show that ALK7 expression in prolactinomas cells is evolutionary conserved between rat and human. More interestingly, our results highlight that tumours showing a robust expression of ALK7 present an increased proliferation as address by Ki67 expression and retrospective analysis of clinical data from 38 patients, presenting ALK7 as an appealing marker of prolactinoma aggressiveness. Beside this observation, our work pinpoints that the expression of prolactin is highly heterogeneous in prolactinoma cells. We further confirm the contribution of ALK7 in these observations and the existence of highly immunoreactive prolactin cells lacking ALK7 expression. Taken together, our observations suggest that Activin signalling mediated through ALK7 could therefore contribute to the hormonal heterogeneity and increased proliferation of prolactinomas.

The clinical–molecular interface of somatostatin, dopamine and their receptors in pituitary pathophysiology, 2009
GABA and Benzodiazepines
Estrogen
Save this Article
Pentobarbital anesthesia during the proestrous afternoon blocks lactotroph proliferation occurring on estrus in female rats. 1995:https://www.ncbi.nlm.nih.gov/pubmed/7664687
- Estradiol stimulates the synthesis and secretion of PRL and lactotroph proliferation, and its long-term administration induces PRL-secreting pituitary tumors. We examined changes in the number of proliferating lactotrophs throughout the estrous cycle in female rats and the involvement of the brain in the regulation of the lactotroph proliferation by anesthetizing with pentobarbital.
Medical Therapy
On the base of molecular data the possible negative effectors of pituitary adenoma cells are:
- dopamine or its analogs
- somatostatin or its analogs (octeotride)
But if we consider that somatostatin (SMS) completely lacks histidine we can imagine an antagonistic action against SMS by histamine (whose level depends on histidine availability) and therefore counteracting the effect of histamine can be a sound approach.
Octreotide
Treatment of multiresistant prolactinomas with a combination of cabergoline and octreotide LAR. 2018 Fulltext
- Abstract
BACKGROUND AND OBJECTIVES:
Dopamine agonist (DA)-resistant prolactinomas are rare but they constitute a real challenge, since there are few therapeutic alternatives left for these patients.
DESIGN AND SETTING:
Proof-of-concept study at a tertiary care, referral center.
PATIENTS AND METHODS:
The studied population consisted of five patients (one female and four males, mean age at diagnosis 23.5 ± 19) with macroprolactinomas with persistent hyperprolactinemia and/or tumor mass despite high doses of cabergoline (CBG) and pituitary surgery, to whom 20 mg monthly of octreotide LAR was added for 6-13 months. Response was evaluated by measuring prolactin (PRL) levels and by magnetic resonance imaging. Immunohistochemistry (IHC) for pituitary hormones, Ki-67, and somatostatin receptor subtypes 2 and 5 was (SSTR2 and 5) was available in two of the subjects.
RESULTS:
The addition of octreotide LAR to ongoing CBG treatment had no effect on either PRL levels or tumor size in three patients. In two of the five patients, combination treatment resulted in a significant reduction in PRL concentrations (from 7643 to 200 ng/mL and from 2587 to 470 ng/mL) as well as in adenoma size (93% reduction). IHC evaluation of tumor samples from two patients (a responder and a non-responder) revealed positive immunostaining for PRL and SSTR5 but not for other pituitary hormones or for SSTR2.
CONCLUSIONS:
The addition of a somatostatin analog to ongoing CBG treatment may be effective in some patients with DA-resistant macroprolactinomas, independently of the adenoma's SSTR expression profile.
Complete clinical and biochemical control with cabergoline and octreotide in a patient with ectopic ACTH syndrome before surgery. 2015 Fulltext
Modica R1, Colao A1, Faggiano A2.
Author information
1
Division of Endocrinology, Department of Clinical Medicine and Surgery, Section of Endocrinology, University Federico II of Naples, Via S. Pansini 5, 80131, Naples, Italy.
2
Division of Endocrinology, Department of Clinical Medicine and Surgery, Section of Endocrinology, University Federico II of Naples, Via S. Pansini 5, 80131, Naples, Italy. afaggian@unina.it.
Efficacy of the combined cabergoline and octreotide treatment in a case of a dopamine-agonist resistant macroprolactinoma. 2011 Fulltext
Fusco A1, Lugli F, Sacco E, Tilaro L, Bianchi A, Angelini F, Tofani A, Barini A, Lauriola L, Maira G, Pontecorvi A, de Marinis L.
Author information
1
Department of Internal Medicine, Università Cattolica del Sacro Cuore, Rome, Italy.
- Abstract
Prolactinomas in males can be voluminous macroadenomas invading the surrounding structures. Medical therapy with dopamine agonists (the treatment of choice for these tumours) may be ineffective in the case of pharmacological resistance. In such cases, even surgical and/or radiation therapy cannot be curative due to the invasive potential of the adenoma. Hence, the appropriate therapeutic approach for these tumours is still a relevant clinical problem for endocrinologists. We report the history of an adolescent male who was diagnosed with a large invasive macroprolactinoma in 2002. He had severe bitemporal hemianopsia and hypopituitarism; prolactin levels at diagnosis were higher than 8,000 ng/ml. Medical therapy with cabergoline was initiated and resulted in decreased prolactin levels but not complete normalisation (maximal tolerated dose 3 mg/day). However, due to the worsening of the visual defect, the patient was operated in July 2004 through the trans-nasal approach and 2 years later through both the transcranial and the transphenoidal approaches. After the second surgery, a significant reduction of tumour mass was obtained. Immunohistochemistry for somatostatin receptors (sstr) subtypes showed a positive staining with the anti-sstr5 antibody. A scintigraphy with 111In-pentetreotide (Octreoscan) revealed a very intense tracer uptake in the sellar region. The administration of long-acting octreotide was initiated. After 12 months of therapy, prolactin levels normalised for the first time. Pituitary MRI did not reveal any tumor progression during a 2-year follow-up. This is a case of an invasive dopamine-resistant macroprolactinoma that was successfully controlled by extensive surgery and combined treatment with cabergoline and octreotide. The expression and functionality of sstr should be investigated in these tumours since a combined therapy with cabergoline and octreotide may be a good therapeutic course of action for select cases.
Treatment with octreotide LAR in clinically non-functioning pituitary adenoma: results from a case-control study. 2012
- Abstract
Surgical cure cannot be achieved in most patients with invasive non-functioning pituitary macroadenoma (NFPA). Short-term residual tumor treatment with somatostatin analogs has produced disappointing results. This prospective case-control study assessed the efficacy of chronic treatment with long acting octreotide (octreotide LAR) on tumor volume in patients harboring post-surgical NFPA residue. The study population comprised 39 patients with NFPAs not cured by surgery. All patients underwent somatostatin receptor scintigraphy at least 6 months after the last surgery. Patients with a positive pituitary level octreoscan at (n = 26) received octreotide LAR (20 mg every 28 days) for ≥ 12 months (mean follow-up 37 ± 18 months) (Treated group). Moreover, a fragment of tumor tissue from patients in the treated group was retrospectively collected to assess the immunohistochemical expression of somatostatin receptor subtypes (SSTRs). The patients with a negative octreoscan (n = 13) formed the control group (mean follow-up 37 ± 16 months). Hormonal, radiological and visual field parameters were periodically assessed. In the treated group, all tumors expressed at least one SSTR subtype. The SSTR5 subtype was the most abundant, followed by SSTR3. The tumor residue increased in five of 26 patients (19%) in the treated group and in seven of 13 controls (53%). Visual field and pituitary function did not change in any patient. This study indicates that SSTR5 and SSTR3 are the most frequently expressed SSTR subtypes in NFPAs and supports a potential role of SSTR subtypes in stabilization of tumor remnant from NFPAs.
Resistance to a long-acting somatostatin analog (SMS 201-995) reversed by surgery in acromegaly. 1990
- Abstract
A 42-year-old woman had acromegaly and a large macroadenoma with supra- and parasellar extension. Her GH levels (median 85 ng/ml, range 63-170 ng/ml) were not responsive to TRH (200 micrograms iv), GHRH (100 micrograms iv) and bromocriptine (Br 2.5 mg po) acute tests; Sm-C level was 8 U/ml. She was treated with octreotide (SMS) (up to 1500 micrograms daily) for 3 months. No changes of clinical, biochemical and radiological findings were seen, therefore she underwent transsphenoidal surgery. After surgery, hypopituitarism and diabetes insipidus appeared: GH levels remained high (median 45 ng/ml; range 37-56 ng/ml), but became responsive to Br acute test. The patient was given SMS again, and this resulted in clinical improvement, marked reduction of GH and Sm-C levels and slight shrinkage of the residual tumor. Speculative hypotheses about this previously unreported phenomenon might be either an excess of both GHRH and somatostatin, caused by a primary increase of dopaminergic tone, or a primary excess only of GHRH; in both cases the surgical lesion of the hypothalamic-pituitary region might have impaired the neurohormones inflow to the residual pituitary and so let SMS and Br exert their inhibitory actions on GH secretion.
Outcome of surgery for acromegaly performed by different surgeons: importance of surgical experience. 205
- Abstract
AIM:
The aim of this study was to evaluate transsphenoidal surgery results in acromegalic patients which were performed not by a single surgeon but by different surgeons.
METHODS:
The study included 30 (M/F: 13/17) patients whose follow-up data were available. Basal or nadir postglucose growth hormone levels of less than 2 ng/ml were accepted as cure criteria. Six of them underwent a further operation due to previous surgical failure.
RESULTS:
Cure was achieved in 33% of patients while hypopituitarism was observed in 10% (3/30) of patients after the first operation. The cure rates were 63% and 15% in patients with microadenomas (n = 11) and macroadenomas (n = 19) respectively (p = 0.042). Only one of the patients (16%) who underwent a second operation achieved remission, while hypopituitarism was observed in five of them (83%). There was no significant difference in the cure rates between the first and second operation, but the risk of hypopituitarism was significantly higher in patients who underwent further surgery (p = 0.008).
CONCLUSION:
The cure rate following surgery is significantly lower in acromegalic patients with macroadenomas than in patients with microadenomas. Cure probability decreases with a further operation, while complication risk increases significantly. Octreotide therapy, which could be used as an alternative therapy to the surgery, revealed high success rates in both microadenomas and macroadenomas. The low cure rates found in this study compared with published series could be attributed to the fact that operations were performed by inexperienced surgeons.
Treatment of nonfunctioning pituitary adenomas: what were the contributions of the last 10 years? A critical view. 2012
- Abstract
OBJECTIVES:
All evidence for treatment and follow-up for nonfunctioning pituitary adenomas (NFMA) is based on observational studies. The objective was to critically review the contributions of the last 10 years on treatment of NFMA.
MATERIALS AND METHODS:
Systematic review.
RESULTS:
Transsphenoidal surgery remains the cornerstone of treatment of NFMA. When compared to the microsurgical procedure, some, but not all, studies favor endoscopy, but endocrinological outcome is not different. Radiosurgery results in a high and durable rate of tumor control, including in those previously treated by conventional radiotherapy, but the risk of developing hypopituitarism is comparable to the risk after conventional radiotherapy. In selected patients without visual field defects, a wait-and-see approach with frequent evaluation of visual fields is possible, without the risk of irreversibly compromising visual function. Tumor progression in NFMA is difficult to predict, but the MIB-1 LI is clinically useful and is indicative of invasiveness, but does not predict recurrence. To date, the potential contribution of other proliferation markers still requires further validation, and effective medical treatment strategies are not available. New features are the role of temozolomide and rapamicin as potential therapeutical targets, combined with octreotide. Although chimeric sst-DA analogues effectively inhibit proliferation in vitro, the effects of these molecules have not yet been evaluated in clinical trials with patients with NFMA.
CONCLUSION:
Surgery, followed by radiotherapy or radiosurgery in case of remnant or recurrence, remains the cornerstone of treatment of NFMA. Currently, medical treatment cannot yet be incorporated in routine clinical practice.
Approach to the incidentally discovered pituitary mass.
Molitch ME1.1996
- Abstract
Incidental pituitary adenomas are being found commonly with our improved neuroradiologic imaging procedures. Screening for hormone oversecretion by these tumors appears to be warranted. For patients with macroadenomas, patients should also be screened for hypopituitarism. In the absence of visual-field abnormalities or hypothalamic/stalk compression, it may be appropriate to observe such patients carefully with repeated MRI scans. A limited amount of data suggest that significant tumor enlargement will occur in < 5% of patients with microadenomas [8,11]. However, all macroadenomas must start out as microadenomas, and so periodic follow-up is indicated to assess for this possibility. Macroadenomas, by their very existence at the time of detection, have already indicated a propensity for growth. Over the limited period of follow-up in the two series reported, significant growth occurred in just over one quarter of the patients with macroadenomas [8,11]. Hemorrhage into such tumors is uncommon, but anticoagulation may predispose to this complication. When there is no evidence of visual-field deficits, an attempt at medical therapy with a dopamine agonist or octreotide is reasonable, realizing that only about 10% of such patients will respond with a decrease in tumor size. Surgery is indicated if there is evidence of tumor enlargement, especially when such growth is accompanied by compression of the optic chiasm, cavernous sinus invasion, or the development of pituitary hormone deficiencies.
Should all patients with acromegaly receive somatostatin analogue therapy before surgery and, if so, for how long? 2014
- Abstract
Current guidelines do not recommend the routine use of somatostatin analogue pretreatment prior to surgery in patients with growth hormone-secreting pituitary tumours. In theory, presurgical use of somatostatin analogues should improve metabolic control and reduce soft tissue swelling, leading to improved anaesthetic outcomes. Shrinkage of tumours prior to surgery might also improve surgical remission rates. Hence, this article addresses the question: Should all patients with acromegaly receive a somatostatin analogue prior to surgery? Clinical trials published before December 2013 were reviewed, although literature in this area remains relatively deficient. We conclude: (i) On the basis of limited data available, somatostatin analogue pretreatment does not improve anaesthetic or immediate postoperative outcomes (i.e. hospital stay, rates of *surgical complications and postoperative pituitary dysfunction). (ii) Somatostatin analogues should be considered in all patients with growth hormone-secreting macroadenomas, including invasive macroadenomas, when the overall surgical remission rate for macroadenomas at the treating centre is below 50%. *Four recent RCTs have demonstrated increased rates of surgical remission using such an approach. (iii) When deemed appropriate, patients should be treated with somatostatin analogues for at least 3 months before surgery; there is currently no evidence that treatment beyond 6 months provides any additional benefit. Patients with minimally invasive macroadenomas are those most likely to benefit in terms of improved surgical remission.
Malignant bronchial carcinoid tumor metastatic to the pituitary in a thyroid carcinoma patient: successful treatment with surgery, radiotherapy and somatostatin analog. 2004
- Abstract
A carcinoid pituitary metastasis is very rare, and is reported scarcely in a few patients. We describe an unusual case of metastatic atypical bronchial carcinoid to the anterior pituitary gland in a 47-year-old male who presented with bitemporal hemianopsia and hypopituitarism. His primary bronchial carcinoid was resected two years previously. Foci of metastatic papillary thyroid carcinoma were also identified in the lung resected for the bronchial carcinoid. He thereby underwent total thyroidectomy followed by radioiodine ablative treatment. Transsphenoidal partial removal of the suprasellar mass was performed, and atypical carcinoid metastasis was identified. He received conventional fractionated sellar radiotherapy, which was supplemented with octreotide (Sandostatin LAR) injections following a positive pituitary uptake on octreotide scan. This treatment suppressed his elevated 5-HIAA urinary excretion to a normal level. His vision has returned to normal and the pituitary mass diminished in size.
Pituitary adenomas in childhood and adolescence. Clinical analysis of 10 cases. 2001
- Abstract
Pituitary adenomas in childhood and adolescence constitute 2-6% of all operated pituitary adenomas. We report the clinical features, treatment and follow-up of 10 pediatric patients affected by pituitary adenomas. All patients underwent clinical evaluation, endocrine tests, magnetic resonance imaging and visual field assessment. Follow-up ranged from 8 to 132 months (median 52.6). All patients were older than 10 years of age; 60% were males. In 50% the initial complaints were headache and/or visual impairment, all except one had clear evidence of endocrine dysfunction. Ninety percent were macroadenomas. According to hormone measurements and immunostaining 50% were prolactinomas, 20% were pure GH-secreting and 30% were non-functioning adenomas. Prolactinomas in two females were successfully treated with cabergoline. The other patients underwent surgery: three prolactinomas are still being treated with dopamine agonists and a GH-secreting adenoma is being treated with octreotide LAR and cabergoline. Two patients were also treated with conventional radiotherapy. Treatments were completely successful in 50% of patients: these have normal hormone secretion, full pubertal development, no significant tumor mass and normal visual field. Hypersecretion of prolactin persists in two cases; partial or complete hypopituitarism is present in four, relevant tumor remnant in another four and impairment of visual field is present in two cases. In conclusion, pediatric adenomas occur mostly in pubertal age, are prevalently macroadenomas and clinically functioning. Medical therapy should be preferred for secreting adenomas, but in some cases, notably prolactinomas in males, surgery and eventual radiotherapy may be needed.
Effect of histamine on the growth of human gastrointestinal tumours: reversal by cimetidine. 1993
- Abstract
The proliferative effects of histamine were examined on the human gastric tumour cell lines; MKN45, the gastrin producing subline, MKN45G, and the colorectal lines; LoVo and C170. The proliferation of MKN45 as assessed by 75[Se] selenomethionine uptake and cell counts was increased by histamine concentrations of 10(-7) and 10(-9) M. Histamine concentrations between 10(-6) and 10(-7) M maximally stimulated MKN45G proliferation which titrated out at lower histamine concentrations. The accumulation of cyclic adenosine 3',5' monophosphate (cAMP) in response to the same histamine concentrations was also increased in the two gastric cell lines. The histamine receptor antagonist, cimetidine (10(-5) M) reversed the histamine stimulated proliferation of both gastric cell lines despite having no effect on basal growth. The proliferation of the colorectal lines was unaffected by histamine. Histamine given locally at the subcutaneous implantation site of the tumour (1 mg/kg/day) increased the growth of MKN45G xenografts in nude mice. This was reversed by coadministration of cimetidine (100 mg/kg/day, given in the drinking water). Cimetidine also inhibited the basal proliferation of MKN45 xenografts. Histamine acting locally may enhance the proliferation of tumours arising within the stomach. Such effects may be blocked by administration of histamine receptor antagonists, such as cimetidine.
Increased therapeutic index of antineoplastic drugs in combination with intracellular histamine antagonists. 1991
- Abstract
L-Histidinol, a protein synthesis inhibitor and structural analogue of L-histidine, has been demonstrated in chemotherapy-treated mice to be cytoprotective to normal stem cells but to enhance cytotoxicity to tumor cells. N,N-Diethyl-2-[4-(phenylmethyl) phenoxy]ethanamine.HCl (DPPE) is an antagonist of recently described microsomal and nuclear intracellular histamine receptors implicated in the mediation of proliferation and modulation of prostaglandin synthesis. DPPE is cytotoxic to tumor cells in vitro and cytoprotective to the gut in vivo. Noting the similar pharmacologic profiles for histidinol and DPPE and the structural resemblance between histidinol and histamine, we tested 1) whether binding to intracellular histamine receptors may be important to the action of histidinol, 2) whether there exists a differential effect of DPPE and histidinol on proliferating normal and transformed or malignant cells, and 3) whether DPPE, like histidinol, protects host cells from the effects of chemotherapy while augmenting tumor cell kill in vivo. It was observed that histidinol does compete at intracellular histamine receptors in isolated microsomes and nuclei, but with significantly lower affinity than DPPE. Nevertheless, for each agent, potency at intracellular histamine receptors correlates with potency to inhibit DNA and protein synthesis, without cytotoxicity, in normal mitogen-stimulated murine lymphocytes and to kill transformed mouse lymphocytes or MCF-7 human breast cancer cells. As demonstrated previously for histidinol (1-2 g/kg), DPPE (4 mg/kg) protected murine bone marrow progenitors from doxorubicin or fluorouracil, while doses of 4-50 mg/kg significantly enhanced the antitumor activity of doxorubicin and daunorubicin in murine models of early cancer. One postulate to explain the effects of intracellular histamine receptor ligands is that intracellular histamine mediates DNA and protein synthesis, possibly through a downward modulation of growth-inhibitory prostaglandin levels. Antagonism of the intracellular action of histamine at intracellular histamine receptors by DPPE or histidinol may result in differential perturbations of growth/eicosanoid metabolism in normal and malignant cells, thus forming the basis of a new approach to chemotherapy.
Histamine: the quintessential mediator. 1996
- Abstract
Histamine is unique in being the only substance described to date which fulfils all of the criteria established by Dale for an inflammatory mediator. Thus, histamine is known to cause the "Triple Response" of Lewis and to act via H1 and H2 receptors to produce vasodilation and increased vascular permeability; elevated levels of histamine are found in inflamed tissue; histamine is produced and stored in mast cells and there are established mechanisms for histamine release via mast cell surface receptors; and antihistamines alleviate the clinical manifestations of histamine release. There have been several recent advances in our understanding of histamine pharmacology and of the pathomechanisms of chronic idiopathic urticaria (CIU), a disease in which histamine plays an important role. Two new histamine receptors have been identified, the inhibitory (H3) receptor and the intracellular (H(ic)) receptor involved in cell proliferation. There is now evidence that mast cell derived histamine release in patients with CIU is due to an autoimmune disease, mediated by autoantibodies to the alpha-subunit of the high affinity IgE receptor on mast cells and basophils. Removal of these autoantibodies by plasmapheresis, or treatment with intravenous immunoglobulins may cause clinical remission. Cyclosporin A has also been found to be of benefit to some patients with CIU probably due to a mast cell "stabilising" effect, leading to reduced release of histamine and other mediators. This article reviews our current knowledge on histamine, its role, receptors and mechanisms for release.
Histamine induces neural stem cell proliferation and neuronal differentiation by activation of distinct histamine receptors. 2008
- Abstract
Histamine has neurotransmitter/neuromodulator functions in the adult brain, but its role during CNS development has been elusive. We studied histamine effects on proliferation, cell death and differentiation of neuroepithelial stem cells from rat cerebral cortex in vitro. RT-PCR and Western blot experiments showed that proliferating and differentiated cells express histamine H(1), H(2) and H(3) receptors. Treatments with histamine concentrations (100 nM-1 mM) caused significant increases in cell numbers without affecting Nestin expression. Cell proliferation was evaluated by BrdU incorporation; histamine caused a significant increase dependent on H(2) receptor activation. Apoptotic cell death during proliferation was significantly decreased at all histamine concentrations, and cell death was promoted in a concentration-dependent manner by histamine in differentiated cells. Immunocytochemistry studies showed that histamine increased 3-fold the number of neurons after differentiation, mainly by activation of H(1) receptor, and also significantly decreased the glial (astrocytic) cell proportion, when compared to control conditions. In summary, histamine increases cell number during proliferative conditions, and has a neuronal-differentiating action on neural stem cells, suggesting that the elevated histamine concentration reported during development might play a role in cerebrocortical neurogenesis, by activation of H(2) receptors to promote proliferation of neural precursors, and favoring neuronal fate by H(1)-mediated stimulation.
Influence of the central histaminergic systems on the pituitary-adrenocortical response to met-enkephalinamide. 1995
- Abstract
A possible involvement of hypothalamic histamine and histamine receptors in the hypothalamic-pituitary-adrenocortical (HPA) activity stimulated by Met-enkephalinamide (DADM) was investigated indirectly by corticosterone secretion in conscious rats. DADM, a delta-opioid receptor agonist, given intracerebroventricularly (i.v.c.) induced a significant increase in the serum corticosterone level, which was considerably reduced by ip or icv pretreatment with naltrexone, an opioid antagonist. Pretreatment with alpha-fluoromethylhistidine (alpha-FMH) 20 mg/kg ip or 50 micrograms icv, an inhibitor of the brain histamine synthesis, drastically reduced the hypothalamic histamine level, did not affect the levels of noradrenaline and dopamine, and almost abolished the DADM-induced corticosterone response. Mepyramine and cimetidine, histamine H1- and H2-receptor antagonists, did not substantially change the corticosterone response to DADM. The present results suggest that DADM stimulates the HPA activity via central delta-opioid receptors. They also indicate that the reduction of the HPA response to DADM by alpha-FMH is connected with significant diminution of hypothalamic histamine, but not noradrenaline or dopamine levels. Central histamine receptors do not mediate the metenkephalinamide-induced HPA stimulation.
The HRH4 rs11662595 mutation is associated with histamine H4 receptor dysfunction and with increased epithelial-to-mesenchymal transition progress in non-small cell lung cancer. 2017
- Abstract
We previously demonstrated that histamine H4 receptor (HRH4) played important roles to suppress epithelial-to-mesenchymal transition (EMT) progress in non-small cell lung cancer (NSCLC). Furthermore, recent investigations suggested that genetic variations in HRH4 gene affected HRH4 function and eventually contributed to certain HRH4-related diseases. However, the relations between polymorphisms in HRH4 gene and NSCLC as well as their underlying mechanisms remain largely uninvestigated. This study aims to investigate the genetic effect of a nonsynonymous HRH4 polymorphism (rs11662595) on HRH4 function and its association with NSCLC both basically and clinically. For basic experiments, A549 cells were transfected with either wild type or rs11662595 mutated HRH4 clone and subjected to both in vitro and in vivo experiments. We showed that rs11662595 significantly decreased the ability of HRH4 to activate Gi protein, which resulted in facilitation of EMT progress, cell proliferation, and invasion behavior in vitro. Moreover, in vivo experiments also showed that rs11662595 attenuated the anti-EMT effects of HRH4 agonist in inoculated nu/nu mice. For clinical experiments, we performed a prospective cohort study among 624 NSCLC patients and further proved that rs11662595 was responsible for the prognosis, degree of malignancy and metastasis of NSCLC. In conclusion, these findings reveal that rs11662595 is a loss-of-function polymorphism that results in dysfunction of HRH4 and attenuates the anti-EMT function of HRH4 in NSCLC, which provides a promising biomarker for prognosis and therapy of NSCLC.
The intracerebroventricularly administered mast cells degranulator compound 48/80 increases the pituitary-adrenocortical activity in rats. 1991
- Abstract
The effect of brain mast cells degranulation by compound 48/80 on the pituitary-adrenocortical activity, measured indirectly through corticosterone secretion, and the involvement of a histaminergic mechanism in that stimulation was investigated in conscious rats. All the drugs were given intracerebroventricularly (icv), histamine antagonists 15 min prior to compound 48/80. Compound 48/80 induced a significant dose- and time-related increase in the serum corticosterone levels. That increase, measured 1 h after administration of compound 48/80, was moderately diminished by icv pretreatment of rats with mepyramine and cimetidine, histamine H1- and H2-receptor antagonists. Three hours after administration of compound 48/80 mast cells of the thalamus and the hypothalamus were completely degranulated. At the same time the thalamus and the whole brain histamine levels were substantially higher than in the saline-treated control rats. The above results suggest that histamine liberated from the brain mast cells and central histamine receptors play a moderate role in increasing the pituitary-adrenocortical activity by compound 48/80.
Establishment and characterization of a new human cultured cell line from a prolactin-secreting pituitary adenoma. 1985
* Abstract
A new human cell line was established from a prolactin (PRL) secreting pituitary adenoma. This cell line, designated as HPA, initially produced and secreted PRL, but the ability was decreased with increasing passage number. After about 30 passages in vitro, these cells had a short doubling time (14 h) and a low plating efficiency (9%). When a minimum of 10(5) cells was injected per mouse, virtually all athymic nude mice developed a slow growing, nonmetastasizing tumor at the injection site about 30 days after injection. PRL production by the HPA cells after Day 150 was demonstrated by immunocytochemistry as well as radioimmunoassay. In addition, cimetidine (10(-4) M) had a significant stimulatory effect on PRL secretion by 4-day-cultured HPA cells. When the HPA cells were incubated in the presence of 5.0 and 10.0 nM bromocriptine, the proliferation rate was inhibited to 53.4 and 25.1% of untreated controls, respectively. On the other hand, the same concentrations of bromocriptine did not affect the proliferation rate of YK cells derived from human immature teratoma of the ovary. In addition, bromocriptine inhibited significantly the growth rate of xenotransplanted HPA but not YK cells. These results suggest that bromocriptine inhibits specifically the proliferation of HPA cells.
histamine prolactin
Neuronal histamine and expression of corticotropin-releasing hormone, vasopressin and oxytocin in the hypothalamus: relative importance of H1 and H2 receptors. 1998
Centrally administered histamine (HA) stimulates the secretion of the pro-opiomelanocortin-derived peptides ACTH and beta-endorphin as well as prolactin.
Nerve growth factor and receptors are significantly affected by histamine stimulus through H1 receptor in pancreatic carcinoma cells. 2010
- Abstract
Nerve growth factor (NGF) as an autocrine or paracrine growth factor plays a critical role in the pathogenesis and progression of human pancreatic cancer. NGF is synthesized as a proform (proNGF) that, when cleaved, releases mature ligand (mNGF). proNGF and mNGF bind to high-affinity tyrosine kinase receptor A (TrkA) and low-affinity receptor p75 to different extents. Histamine is a potent stimulator of NGF in the inflammatory lesion as determined by ELISA. This has generally been attributed to the accumulation of mNGF. To determine the effect of histamine on nerve growth factor/receptor expression in human pancreatic cancer, the present study explored intracellular and extracellular NGF production and p75 and TrkA membrane receptor expression in the PANC-1, KMP-6 and PK-1 cell lines. Histamine enhanced NGF secretion and mRNA expression in PANC-1 and KMP-6 cells, but not in PK-1 cells. proNGF was revealed using Western blotting to be the predominant form of NGF, but was significantly reduced by histamine. p75 receptor binding was increased with histamine treatement, but no significant alteration was observed for TrkA. Proliferating cell nuclear antigen (PCNA), an important indicator of cell proliferation, was significantly reduced by histamine stimulation. H1 and H2 receptors were both observed in the pancreatic cancer cells, and the alterations induced by histamine were counteracted by H1 receptor antagonist pyrilamine; however, the H2 receptor subtype was excluded from this process. These results suggest that histamine induces distinct nerve growth factor/receptor responsiveness via H1 receptor-induced signaling, thus affecting pancreatic cancer cell proliferation.
H1 inhibitors have anti-proliferative effect?
Effect of estrogen and neuroleptics on prolactin secretion and immunoreactive prolactin cells. 1996
The use of estrogen and dopamine receptor antagonists is associated with elevated prolactin levels and, in rats, chronic estrogen treatment is also associated with lactotroph proliferation
Constitutive tyrosine phosphorylation of ErbB-2 via Jak2 by autocrine secretion of prolactin in human breast cancer. 2000
Our results indicate that autocrine secretion of PRL stimulates tyrosine phosphorylation of ErbB-2 by Jak2, provides docking sites for Grb2 and stimulates Ras-MAP kinase cascade, thereby causing unrestricted cellular proliferation.
histamine+receptor+h1+antagonist+prolactin
Cetirizine H1 inhibitor
Cetirizine++cell+proliferation
DHEA
Suppressive effects of dehydroepiandrosterone and the nuclear factor-kappaB inhibitor parthenolide on corticotroph tumor cell growth and function in vitro and in vivo. 2006
Dehydroepiandrosterone (DHEA) is believed to have an anti-tumor effect, as well as anti-inflammatory, antioxidant, and anti-aging effects. To clarify the possible inhibitory action of DHEA on pituitary tumor cells, we tested the effects of DHEA, alone or in combination with the nuclear factor-kappaB (NF-kappaB) inhibitor parthenolide (PRT), on AtT20 corticotroph cell growth and function both in vitro and in vivo. We found that, in vitro, DHEA and PRT had potent inhibitory effects on pro-opiomelanocortin and NF-kappaB-dependent gene expression. They also suppressed the transcription activity of survivin, a representative anti-apoptotic factor, and induced apoptosis in this cell line. Furthermore, using BALB/C nude mice with xenografts of AtT20 cells in vivo, we found that the combined administration of DHEA and PRT significantly attenuated tumor growth and survivin expression. The treatment also decreased the elevated plasma corticosterone levels and ameliorated the malnutrition induced by tumor growth. Altogether, these results suggested that combined treatments of DHEA and PRT potently inhibit the growth and function of corticotroph tumor cells both in vitro and in vivo. This effect may, at least partly, be caused by the suppressive effects of these compounds, such as survivin and other inhibitor of apoptosis proteins, on NF-kappaB-mediated gene transcription.