A substantial body of evidence shows an association between an increased risk of suicide and naturally low or therapeutically lowered serum cholesterol.
1)Cholesterol

Cholesterol is an organic chemical substance classified as a waxy steroid of fat.
Function
- Cholesterol is required to build and maintain membranes; it modulates membrane fluidity over the range of physiological temperatures. Through the interaction with the phospholipid fatty acid chains, cholesterol increases membrane packing, which reduces membrane fluidity. In this structural role, cholesterol reduces the permeability of the plasma membrane to neutral solutes, protons, (positive hydrogen ions) and sodium ions.
- Within the cell membrane, cholesterol also functions in intracellular transport, cell signaling and nerve conduction.
• Cholesterol is essential for the structure and function of invaginated caveolae and clathrin-coated pits, including caveola-dependent and clathrin-dependent endocytosis.
• Recently, cholesterol has also been implicated in cell signaling processes, assisting in the formation of lipid rafts in the plasma membrane. Lipid raft formation brings receptor proteins in close proximity with high concentrations of second messenger molecules.
• In many neurons, a myelin sheath, rich in cholesterol, since it is derived from compacted layers of Schwann cell membrane, provides insulation for more efficient conduction of impulses.
- Within cells, cholesterol is the precursor molecule in several biochemical pathways.
• In the liver, cholesterol is converted to bile, which is then stored in the gallbladder.
• Cholesterol is an important precursor molecule for the synthesis of vitamin D and the steroid hormones, including the adrenal gland hormones cortisol and aldosterone, as well as the sex hormones progesterone, estrogens, and testosterone, and their derivatives.
- Some research indicates cholesterol may act as an antioxidant.
Hypercholesterolemia
Hypercholesterolemia is the presence of high levels of cholesterol in the blood.
Although cholesterol is important and necessary for human health, high levels of cholesterol in the blood have been linked to damage to arteries and cardiovascular disease.
Elevated cholesterol in the blood involves abnormalities in the protein particles which transport all fat molecules, including cholesterol, within the water of the bloodstream. This may be related to diet, increased body fat, genetic factors (such as LDL receptor mutations in familial hypercholesterolemia) and the presence of other diseases such as diabetes and an underactive thyroid. The type of hypercholesterolemia depends on which type of particle (such as low-density lipoprotein) is present in excess.
Some have proposed that hypercholesterolemia can be treated by reducing dietary cholesterol intake. Administration of certain medications which reduce cholesterol production or absorption is usually more effective. Rarely other treatments including surgery (for particular severe subtypes) are performed.
For those at high risk a combination of lifestyle modification and statins has been shown to decrease mortality.
2)Studies
Although large primary prevention trials have established that lowering serum cholesterol concentrations by either dietary or pharmacologic intervention reduces incidence of coronaric heart disease events […] no study provided evidence that lowering cholesterol concentrations extends survival. The failure of intervention to affect total mortality in primary prevention trials is due in part to a trend in several studies toward higher rates of deaths from cancer and from accidents and suicide among groups receiving treatment to lower cholesterol concentrations.
The results of Muldoon’s study showed that mortality from coronary heart disease tended to be lower in men receiving interventions to reduce cholesterol concentrations compared with mortality in control subjects (p=0,06), although total mortality was no affected by treatment. No consistent relation was found between reduction of cholesterol concentrations and mortality from cancer, but there was a significant increase in death not related to illness (death from accident, suicide, or violence) in groups receiving treatment to lower cholesterol concentration relative to controls (p=0,004).
Lowering cholesterol concentrations and mortality: a quantitative review of primary prevention trials, 1990
In 1996 the analysis of results from some long-term epidemiological studies shows an excess of suicides and violent death cases among persons with low baseline total serum cholesterol level and in those in whom this level was lowered by means of pharmacotherapy or dieting. Such relationship was most evident in patients with depression. In some populations, an association between low total cholesterol level and the tendency to aggressive behavior was also found. Higher intensity of aggression was also observed in animals receiving low-cholesterol diet.
Low concentration level of total serum cholesterol as a risk factor for suicidal and aggressive behavior, 1996
There have been some reports that changes in serum lipid composition may be related to suicide, major depression and immune-inflammatory responses. In 1997 findings suggest that major depression is accompanied by reduced formation of cholesteryl esters and perhaps by impairment of reverse cholesterol transport. The latter is reportedly accompanied by lower serum high-density lipoprotein cholesterol(HDL-C).
Serum HDL-C and total cholesterol, as well as the HDL-C/cholesterol ratio, were significantly lower in subjects with major depression than in normal controls. Serum HDL-C levels were significantly lower in depressed men who had at some time made serious suicidal attempts than in those without such suicidal behaviour. Serum HDL-C levels were significantly and negatively correlated with the (CD4+/CD8+) T-cell ratio, and positively correlated with serum Alb and Zn.
These results suggest that
1) lower serum HDL-C levels are a marker for major depression and suicidal behaviour in depressed men,
2) lower serum HDL-C levels are probably induced by the immune/inflammatory response in depression and
3) there is impairment of reverse cholesterol transport from the body tissues to the liver.
Lower serum high-density lipoprotein cholesterol (HDL-C) in major depression and in depressed men with serious suicidal attempts: relationship with immune-inflammatory markers, 1997
In 2000 there was a study to determine the level of total cholesterol and LDL-cholesterol in blood samples, in which putative correlations between the level of total cholesterol and severity of depressive symptoms and between total serum cholesterol and LDL-cholesterol and suicidal risk were evaluated.
The following parameters were evaluated: total serum cholesterol and LDL-cholesterol, T3, T4, TSH, ALT, AST, proteinogram. In all depressed patients with acute depression symptoms, low levels of total cholesterol and LDL-cholesterol were shown.
The level of total cholesterol 160 mg/dl or less and the level of LDL-cholesterol 100 mg/dl or less were observed in persons with suicidal behavior only (S+ and AS).
Low total cholesterol and LDL-cholesterol levels in persons in the acute period of major depression provided a useful parameter of suicide risk.
A significant statistical correlation between the low level of total cholesterol and suicidal ideation was also found (r = 0.82, p < 0.05) as well as between the low level of serum total cholesterol and severity of depression, as evaluated by HAMD-S (r = 0.27, p < 0.05). During the remission of depressive symptoms, total cholesterol level and LDL-cholesterol increased significantly (p < 0.05). Low total cholesterol and LDL-cholesterol levels in remission in persons with the diagnosis of recurrent major depression may help to estimate the risk of suicidal behavior in the next depressive disorder. Possibly, low level of serum total cholesterol is a stable feature in some persons with recurrent major depression, probably dependent on their predisposition to autoaggression and presence of depressive disorder.
Levels of serum total cholesterol and LDL-cholesterol in patients with major depression in acute period and remission, 2000
Many confounding factors, e.g. poor health, depression and loss of appetite may play a role in the apparent relationship between serum cholesterol levels and suicide. Two separate phenomena should be considered:
-lowering total cholesterol and
-low total cholesterol.
According to an Italian study in 2000 available evidence does not seem to substantiate the view that large-scale intervention to reduce cholesterol concentrations could lead to more violent and aggressive behaviour, and generally greater unhappiness. In recent trials using statin treatment, there were slightly fewer deaths from accidents and suicide in the treated group compared with the placebo group.
The association of low serum cholesterol with depression and suicidal behaviours: new hypotheses for the missing link, 2000
Serum cholesterol levels were significantly lower in suicide attempters than in controls. After gender stratification, the difference remained significant in men, but not in women.
Low plasma cholesterol levels in suicidal males: a gender- and body mass index-matched case-control study of suicide attempters and nonattempters,2007
Low cholesterol levels were not associated with increased suicide risk but with a decreased risk in US men.
Lack of replication of the association of low serum cholesterol and attempted suicide in another country raises more questions,2011
Many studies have demonstrated an association between suicidal behavior and low levels of total serum cholesterol. This association has mainly been reported in men. A case-control study was undertaken in 2011 to assess the association between serum cholesterol level and suicide attempts in both genders.
After adjustment for age, cholesterol level was significantly lower (p<0.01) in suicide attempters than in non-attempters and controls for both genders. Male non-suicide attempters had similar cholesterol levels to controls (p=0.7), but the levels in female non-attempters were significantly higher (p=0.004). The proportion of suicide attempters in the lowest cholesterol level quartile (51.3% of men, 40.1% of women) was significantly higher than that in the highest quartile (8.1% of men, 12.4% of women). For triglyceride level, no difference was found between the three groups, suggesting that this association was not due to malnutrition linked to depression.
Total serum cholesterol levels measured at admission may be a useful biological marker of suicidal risk.
Measurement of total serum cholesterol in the evaluation of suicidal risk, 2011
3) Hypothesis
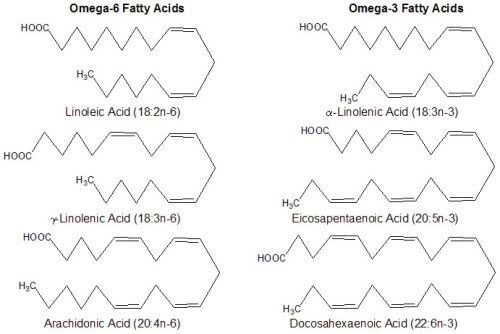
Polyunsatured fatty acids are made out of a hydrocarbonated chain of variable length with several double bonds.
The position of the first double bond (omega) differentiates polyunsatured omega 3 fatty acids (for example: alpha-linolenic acid or alpha-LNA) and polyunsatured omega 6 fatty acids (for example: linoleic acid or LA). These two classes of fatty acids are said to be essential because they cannot be synthetised by the organism and have to be taken from alimentation.
The omega 3 are present in linseed oil, nuts, soya beans, wheat and cold water fish whereas omega 6 are present in maize, sunflower and sesame oil.
Fatty acids are part of phospholipids and, consequently, of all biological membranes. The membrane fluidity, of crucial importance for its functioning, depends on its lipidic components. Phospholipids composed of chains of polyunsatured fatty acids increase the membrane fluidity because, by bending some chains, double bonds prevent them from compacting themselves perfectly.
Membrane fluidity is also determined by the phospholipids/free cholesterol ratio, as cholesterol increases membrane viscosity.
A diet based on a high proportion of essential polyunsatured fatty acids (fluid) would allow a higher incorporation of cholesterol (rigid) in the membranes to balance their fluidity, which would contribute to lower blood cholesterol levels.
Brain membranes have a very high content in essential polyunsatured fatty acids for which they depend on alimentation. Any dietary lack of essential polyunsatured fatty acids has consequences on cerebral development, modifying the activity of enzymes of the cerebral membranes and decreasing efficiency in learning tasks.
The prevalence of depression seems to increase continuously since the beginning of the century. Though different factors most probably contribute to this evolution, it has been suggested that it could be related to an evolution of alimentary patterns in the Western world, in which polyunsatured omega 3 fatty acids contained in fish, game and vegetables have been largely replaced by polyunsatured omega 6 fatty acids of cereal oils.
Lipids, depression and suicide, 2003
A hypothesis was discussed, postulating the connection between low cholesterol level and lower activity of central serotonergic structures responsible for the inhibition of impulsive behavior.
Low concentration level of total serum cholesterol as a risk factor for suicidal and aggressive behaviour, 1996
Data support the hypothesis that cholesterol reduction may contribute to the serotonergic abnormalities that have been postulated in suicidal subjects.
In 2002 it was hypothesised that a decreased consumption of polyunsaturated fatty acids, especially omega-3 fatty acids, may be a risk factor for depression and suicide.
We do not have sufficient evidence that cholesterol-lowering therapies increase the risk of depression and suicide, but increasing the dietary intake of omega-3 fatty acids may increase central serotonergic activity and reduce impulsive and aggressive behaviours.
Cholesterol, essential fatty acids, and suicide, 2003
4) Conclusions
The interrelationships of cholesterol, cholesterol-lowering medications, depressive disorders, and the risk of suicide are more likely to be multi-directional:
- On the one hand, low cholesterol may have direct effects on mood and suicidal behaviors.
- On the other hand, psychological conditions and the medications for treatment may influence eating and exercise habits, and subsequently cholesterol levels.
There is also likelihood that cholesterol might be a bystander of the association between suicide and other factors. Overall, the association not only represents a public health concern, is indeed a scientific challenge.
Epidemiological link between low cholesterol and suicidality: a puzzle never finished, 2011