Francesco Pegoraro, Marco Verri
Definition
Post traumatic stress disorder
is an anxiety disorder characterized by symptoms of re-experiencing the trauma such as flashbacks, intrusions or nightmares, avoidance behaviours and hyper-arousal persisting for more then one month post experiencing or witnessing extreme traumatic events involving actual or perceived threat of death or serious injury or threat to one’s physical integrity " (as defined by the American psychiatric association 1994)
PTSD is common in victims of physical or sexual assaults (often on a chronic basis, as domestic violence), in severe physical injury, such as that resulting from a car crash, and in combatants in armed conflicts.
Indeed, more than 10% of US Army soldiers returned from deployment suffer from PTSD or from major depression, both of which increase the risk of suicide.
Another study estimated at 7% the lifetime prevalence of PTSD in the US general population,
but it grows up to 35% in people who experienced the war in Bosnia and Herzegovina.
Posttraumatic stress disorder in a serbian community: seven years after trauma exposure., 2013
The recent military operations in Iraq and Afghanistan, which involved the first sustained ground combat undertaken by the United States since the war in Vietnam has raised important questions about the effect of such experience on the mental health of members of the military services who have been deployed there. Studies conducted just before the military operations in Iraq and Afghanistan demonstrated that many of all U.S. military service members on active duty receive treatment for a mental disorder each year. This implies that given the on-going military operations in Iraq and Afghanistan, mental disorders are likely to remain an important health care concern among those serving there.

Anatomy and Biochemical mechanisms
Anatomically, there are two brain regions involved in the onset of the disorder: the hippocampus and the amygdale.
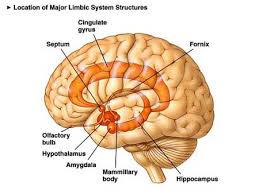 Hippocampus is associated with the ability to play memories in the correct contest of space and time, and with the ability to recall the memory. Since high stress suppresses it, this could be the cause of flashbacks that often plague PTSD patients.
Hippocampus is associated with the ability to play memories in the correct contest of space and time, and with the ability to recall the memory. Since high stress suppresses it, this could be the cause of flashbacks that often plague PTSD patients.
Amygdala is known to be strongly involved in the formation of emotional fear-related memories and this process becomes even more relevant in PTSD patients.
Stress, memory and the amygdala, 2009
Memory consolidation is induced by changing in the morphological structure of the dendritic spines. The mechanisms involved are the creation of spines and their transformation in order to reduce the electrical resistance, and therefore facilitate the synapses.
 There is a specific biochemical mechanism that makes possible the ability to keep memories: in a normal situation, the hyper-stimulation of the cell induces the reduction of its activity and the reduction of the neurotransmitter release; however in the hippocampus and amygdale neurons hyper-stimulation activates the serotonin (5-HT) transmission pathway. This is followed by an increased concentration of cAMP and the activation of the PKA kinase, leading to calcium release. The final consequence is a mayor activation of the memory consolidation processes.
There is a specific biochemical mechanism that makes possible the ability to keep memories: in a normal situation, the hyper-stimulation of the cell induces the reduction of its activity and the reduction of the neurotransmitter release; however in the hippocampus and amygdale neurons hyper-stimulation activates the serotonin (5-HT) transmission pathway. This is followed by an increased concentration of cAMP and the activation of the PKA kinase, leading to calcium release. The final consequence is a mayor activation of the memory consolidation processes.
The biochemical features involved in the PTSD are related to an over-activation of the sympathetic system. This is translated into a fight or flight over-response which consequently leads to high secretion of catecholamine. Among them epinephrine (Eph) and norepinephrine (NE) are the most relevant.
These aspects have been deeply examined in the section of the site regarding Sex and sleep in post traumatic stress disorder
What appears unusual in this fight or flight response is the low level of cortisol, which normally has an anti-stress and anti-inflammatory effects.
Many studies have provided evidences about such significant connection between low cortisol and post traumatic stress disorder.
Salivary cortisol, posttraumatic stress symptoms, and general health in the acute phase and during 9-month follow-up, 2001
In stress-related anxiety disorders, including PTSD, the Neuropeptide Y (NPY) has been proposed as a stress resilience factor, because it regulates stress and anxiety. It has been hypothesized that in central nervous system NPY is deregulated in PTSD and sought to redress the absence of central NPY data in the disorder.
Low Cerebrospinal Fluid Neuropeptide Y Concentrations in Posttraumatic Stress Disorder, 2009
Traumatic events are memorized as a result of the capacity of synaptic connections and the surrounding matrix to undergo experience-dependent functional or morphological changes. Extracellular proteases are strategically poised to remodel the neuron–extracellular-matrix interface and facilitate fear and anxiety. Eph-receptor tyrosine kinases constitute an important group of molecules subject to modulation by extracellular proteases.
Moreover, the effects of Neuropsin, a serine protease uniquely positioned to facilitate stress-induced plasticity due to its high expression in the amygdala and hippocampus might be also relevant.
In particular, stress elicits Neuropsin-dependent cleavage of EphB2 in the amygdale. This, on turn, results in dissociation of EphB2 from the NR1 subunit of the NMDA receptor and promotes membrane turnover of EphB2 receptors. Dynamic EphB2–NR1 interaction enhances NMDA receptor current, induces Fkbp5 gene expression and enhances behavioural signatures of anxiety.
Neuropsin cleaves EphB2 in the amygdala to control anxiety, 2011
Genetics
THE GENE FKBP5
As above reported, Neuropsin induces transcription of FKBP5 gene, encoding for a co-chaperone protein influencing glucocorticoid receptor sensitivity; the protein encoded by this gene is a member of the immunophilin protein family, which play a role in immunoregulation and basic cellular processes involving protein folding and trafficking.This encoded protein is a cis-trans prolyl isomerase that binds to the immunosuppressants FK506 and rapamycin. It is thought to mediate calcineurin inhibition. Such event has been found associated with PTSD plasma cortisol and PTSD severity among survivors of the World Trade Centre attacks and specific types of hypothalamic-pituitary-adrenal axis dysfunctions within PTSD (1).
The FKBP5 gene has been also found to have multiple polyadenylation sites and it is statistically associated with a higher rate of depressive disorders.
Protein Aminoacids Percentage

THE GENE PRKCA
Moreover, the PRKCA gene that encodes for an enzyme called protein kinase C-alpha, plays an important role in the formation of emotional memories. However, a recent study shows that this gene isn’t only connected with a better memory but also with an increased risk of developing PTSD. Indeed, when the distribution of the A allele in a group of 347 survivors of the 1994 Rwandan genocide who had fled the civil war and were living in a Ugandan refugee camp was examined, they found that all had experienced multiple traumatic events during the civil war, but only 134 of them had been diagnosed with PTSD. The A allele was significantly over-represented in those with a diagnosis of PTSD and this clearly underlines how it is an important predictive factor for the disorder (1).
Protein Aminoacids Percentage

More recently a number of relevant genes involved in the PTSD have been identified:
At this regard, evidence has been provided for the serotonin transporter (5-HTT) gene promoter region (5-HTTLPR) to be associated with symptoms related to acute stress disorder, as well as with the PTSD severity score and PTSD as a categorical nosological entity.
Association of variation in the serotonin 2A receptor (5-HT2A) gene has been described as a risk factor for PTSD in a trauma-exposed sample
Furthermore, it has been reported that variants of corticotrophin releasing hormone type 1 receptor gene (CRHR1) predict the onset of posttraumatic stress symptoms and the course of the disease.
Finally, a variant in a putative oestrogen response element within the ADCYAP1R1 gene, encoding for the receptor of the pituitary adenylate cyclase-activating polypeptide (PACAP), was found associated with PTSD, particularly in females.
Further evidences have been provided for variation in genes involved in the dopaminergic system to increase vulnerability to PTSD: association with PTSD has been reported for the catechol-O-methyltransferase (COMT) gene and the dopamine D2 receptor (DRD2) gene , with support for DRD2 variation to specifically mediate severe co-morbid psychopathology (anxiety, depression) and social dysfunction in PTSD subjects
Treatments
Since the prevalence of the PTSD is increasing efforts have been made to discover and develop specific therapeutic strategies. Currently available treatments have been exploited in PTSD patients:

1) Selective serotonin reuptake inhibitors (SSRIs ) are a kind of antidepressant drug able to attenuate sad and worried feelings. They appear to be useful, and in some cases they are very effective. SSRIs include citalopram (Celexa), fluoxetine (such as Prozac), paroxetine (Paxil), and sertraline (Zoloft). Depression is often linked to the lack of the serotonin . Therefore, SSRIs are the right therapeutics to raise its level in the brain.
2) Monoamine oxidase inhibitors (MAOIs) such as Fenelzine and Moclobemide.
These drugs are currently used to treat symptoms of revival and intrusion, as well as depression and panic attacks, frequently connected to PTSD.
3) Psychotherapy is used in the treatment of PTSD to help patients to address and manage painful memories until they no longer cause disabling symptoms. This starts after establishing a safe relationship between the patient and therapist and involves gradually working through the traumatic event and the patient's reactions to it, validating the patient's experience and repairing damage done to their identity.
Eye movement desensitization and reprocessing (EMDR) is a specialized form of psychotherapy that is used primarily for treating PTSD and its associated conditions, including depression. EMDR typically is integrated into a conventional psychotherapy regimen and is not used alone to treat PTSD. The theory behind EMDR is that stimulated rapid eye movement may help in the psychological processing of trauma. It is thought that the day's events and our reactions to them are processed during REM sleep. In a controlled EMDR session, a stimulus such as moving light is used to induce rapid eye movement. The EMDR Institute states that almost 1,000,000 people had been treated since the 1995, and different degree of improvement has been obtained. Some, but not all, studies documented an improvement after relatively few interventions.
New therapeutics are currently under investigation:
- The use of morphine may protect against the subsequent development of PTSD after serious injury. In fact, the use of morphine is associated with a significantly reduced risk of PTSD development in injured military personnel. It has been shown that it may be a first-line defence when exploited after injury, during resuscitation and early trauma care.
Morphine Use after Combat Injury in Iraq and Post-Traumatic Stress Disorder, 2010
- Even propanolol has been repeatedly associated with a reduction of the consolidation of bad memories. It is a β-adrenergic blocker that, if given within hours of a psychologically traumatic event reduces physiologic responses during subsequent mental imagery of the event. We provide the example of a research group which tested the effect of propranolol given after the retrieval of memories of past traumatic events. The results clearly underline a positive effect of this treatment.
Effect of post-retrieval propranolol on psychophysiologic responding during subsequent script-driven traumatic imagery in post-traumatic stress disorder, 2007