Definition
Social anxiety disorder, also known as social phobia, is an anxiety disorder characterized by intense fear in social situation causing considerable distress and impaired ability to function in at least some parts of daily life. Generalized social anxiety disorder typically involves a persistent, intense, chronic fear of being judged by others and of being embarrassed or humiliated by one's own actions. These fears can be triggered by perceived or actual scrutiny from others. While the fear of social interaction may be recognized by the person as excessive or unreasonable, overcoming it can be quite difficult. (Anxiety & Panic Disorders Health Center).

Symptoms
Cognitive aspects
social phobics experience dread over how they will be presented to others.They may be overly self-conscious, pay high self-attention after the activity, or have high performance standards for themselves. According to the social psychology theory of self-presentation, a sufferer attempts to create a well-mannered impression on others but believes he or she is unable to do so. Many times, prior to the potentially anxiety-provoking social situation, sufferers may deliberately go over what could go wrong and how to deal with each unexpected case. After the event, they may have the perception they performed unsatisfactorily. Consequently, they will review anything that may have possibly been abnormal or embarrassing. These thoughts do not just terminate soon after the encounter, but may extend for weeks or longer. Thoughts are often self-defeating and inaccurate. Those with social phobia tend to interpret neutral or ambiguous conversations with a negative outlook and many studies suggest that socially anxious individuals remember more negative memories than those less distressed. (Psychological Medicine ,2003)
Behavioural aspects
Those who suffer from social anxiety disorder are afraid of being judged by others in society. People who suffer from this disorder may behave a certain way or say something and then feel embarrassed or humiliated after. Therefore, they choose to isolate themselves from society to avoid such situations. They may also feel uncomfortable meeting people they do not know and act distant when they are with large groups of people. In some cases they may show evidence of this disorder by not making eye contact or blushing when someone is talking to them.
Physiological aspects
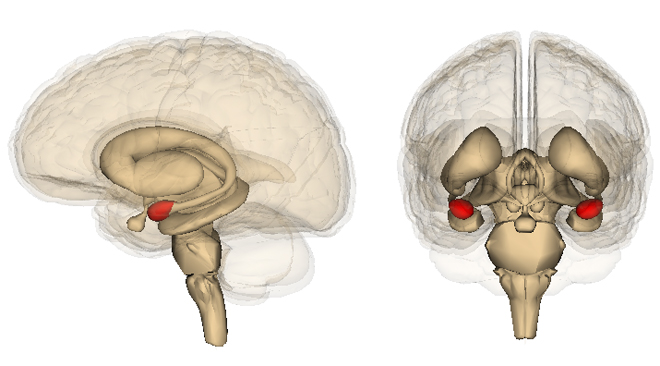
In adults, it may be tears as well as experiencing excessive sweating, nausea, difficulty breathing, shaking, and palpitations as a result of the fight-or-flight response. The walk disturbance (where a person is so worried about how they walk that they may lose balance) may appear, especially when passing a group of people. Blushing is commonly exhibited by individuals suffering from social phobia. These visible symptoms further reinforce the anxiety in the presence of others. A 2006 study found that the area of the brain called the amygdala, part of the limbic system, is hyperactive when patients are shown threatening faces or confronted with frightening situations. They found that patients with more severe social phobia showed a correlation with the increased response in the amygdala.( Studying Brain Activity Could Aid Diagnosis Of Social Phobia , 2006)
Comorbidity
There is a high degree of comorbidity with other psychiatric disorders. Social phobia often occurs alongside low self-esteem and clinical depression, perhaps due to a lack of personal relationships and long periods of isolation from avoiding social situations. To try to reduce their anxiety and alleviate depression, people with social phobia may use alcohol or other drugs, which can lead to substance abuse. It is estimated that one-fifth of patients with social anxiety disorder also suffer from alcohol dependence. The most common complementary psychiatric condition is clinical depression. In a sample of 14,263 people, of the 2.4 percent of persons diagnosed with social phobia, 16.6 percent also met the criteria for clinical depression. Besides depression, the most common disorders diagnosed in patients with social phobia are panic disorder (33 percent), generalized anxiety disorder (19 percent), post-traumatic stress disorder (36 percent), substance abuse disorder (18 percent), and attempted suicide (23 percent).In one study of social anxiety disorder among patients who developed comorbid alcoholism, panic disorder, or depression, social anxiety disorder preceded the onset of alcoholism, panic disorder and depression in 75 percent, 61 percent, and 90 percent of patients, respectively. Avoidant personality disorder is also highly correlated with social phobia. Patients who suffer from both alcoholism and social anxiety disorder are more likely to avoid group-based treatments and are more likely to relapse compared to people who do not have both disorders simultaneously. (The heavy burden of psychiatric comorbidity , 2010)
Genetic and family factors
It has been shown that there is a two to threefold greater risk of having social phobia if a first-degree relative also has the disorder. This could be due to genetics and/or due to children acquiring social fears and avoidance through processes of observational learning or parental psychosocial education. Studies of identical twins brought up (via adoption) in different families have indicated that, if one twin developed social anxiety disorder, then the other was between 30 percent and 50 percent more likely than average to also develop the disorder. A related line of research has investigated 'behavioural inhibition' in infants – early signs of an inhibited and introspective or fearful nature. Studies have shown that around 10–15 percent of individuals show this early temperament, which appears to be partly due to genetics. Some continue to show this trait in to adolescence and adulthood, and appear to be more likely to develop social anxiety disorder. (Vulnerability factors among children at risk for anxiety disorders , 1999)
Evolutionary context
An evolutionary explanation of anxiety is that it reflects an in-built 'fight or flight' system, which errs on the side of safety. One line of research suggests that specific dispositions to monitor and react to social threats may have evolved, reflecting the vital and complex importance of social living and social rank in human ancestral environments. Charles Darwin originally wrote about the evolutionary basis of shyness and blushing, and modern evolutionary psychology and psychiatry also addresses social phobia in this context. It has been hypothesized that in modern day society these evolved tendencies can become more inappropriately activated and result in some of the cognitive 'distortions' or 'irrationalities' identified in cognitive-behavioral models and therapies Another evolutionary explanation, applicable to social situation with strangers, is that in an ancestral environment characterized by small bands in which all individuals were known to one another, it was usually very dangerous to be confronted by a large group of staring, non-kin, unknown, and not smiling strangers. (Evolution and social anxiety, 2001)
Neural mechanisms
Dopamin
Sociability is closely tied to dopamine neurotransmission. Misuse of stimulants like amphetamines to increase self-confidence and improve social performance is common. In a recent study a direct relation between social status of volunteers and binding affinity of dopamine D2/3 receptors in the striatum was found. Other research shows that the binding affinity of dopamine D2 receptors in the striatum of social anxiety sufferers is lower than controls. Some other research shows an abnormality in dopamine transporter density in the striatum of social anxiety sufferers. Studies have shown high prevalence of social anxiety in Parkinson's disease and schizophrenia. In a recent study, social phobia was diagnosed in 50% of Parkinson's disease patients. Other researchers have found social phobia symptoms in patients treated with dopamine antagonists like haloperidol, emphasizing the role of dopamine neurotransmission in social anxiety disorder.Also, concentration problems, mental and physical fatigue, anhedonia and decreased self-confidence are seen in those with social anxiety disorder.(Low dopamine D(2) receptor binding potential in social phobia , 2000), (Dopamine reuptake site densities in patients with social phobia , 1997) 
Other neurotransmitters
Some scientists hypothesize that social phobia is related to an imbalance of the brain chemical serotonin. A recent study reports increased serotonin transporter binding in psychotropic medication-naive patients with generalized social anxiety disorder. Although there is not much evidence of abnormality in serotonin neurotransmission, the limited efficacy of medications which affect serotonin levels may indicate the role of this pathway. Paroxetine and sertraline are two SSRIs that have been confirmed by the FDA to treat social anxiety disorder. Some researchers believe that SSRIs decrease the activity of the amygdala. There is also increasing focus on other candidate transmitters, e.g. norepinephrine and glutamate, which may be over-active in social anxiety disorder, and the inhibitory transmitter GABA, which may be under-active. (Neurobiological mechanisms of social anxiety disorder , 2001)
Brain areas
The amygdala is part of the limbic system which is related to fear cognition and emotional learning. Individuals with social anxiety disorder have been found to have a hypersensitive amygdala, for example in relation to social threat cues (e.g. someone might be evaluating you negatively), angry or hostile faces, and while just waiting to give a speech. Recent research has also indicated that another area of the brain, the anterior cingulate cortex, which was already known to be involved in the experience of physical pain, also appears to be involved in the experience of 'social pain', for example perceiving group exclusion.
Prevalence
The National Comorbidity Survey of over 8,000 American correspondents in 1994 revealed 12-month and lifetime prevalence rates of 7.9 percent and 13.3 percent, respectively; this makes it the third most prevalent psychiatric disorder after depression and alcohol dependence and the most apparent of the anxiety disorders. According to U.S. epidemiological data from the National Institute of Mental Health, social phobia affects 5.3 million adult Americans in any given year. Cross-cultural studies have reached prevalence rates with the conservative rates at 5 percent of the population. However, other estimates vary within 2 percent and 7 percent of the U.S. adult population.
The mean onset of social phobia is 10 to 13 years. Onset after age 25 is rare and is typically preceded by panic disorder or major depression. Social anxiety disorder occurs more often in females than males, but men are more likely to seek help. The prevalence of social phobia appears to be increasing among white, married, and well-educated individuals. As a group, those with generalized social phobia are less likely to graduate from high school and are more likely to rely on government financial assistance or have poverty-level salaries. Surveys carried out in 2002 show the youth of England, Scotland, and Wales have a prevalence rate of 0.4 percent, 1.8 percent, and 0.6 percent, respectively. The prevalence of self-reported social anxiety for Nova Scotians older than 14 years was 4.2 percent in June 2004 with women (4.6 percent) reporting more than men (3.8 percent). In Australia, social phobia is the 8th and 5th leading disease or illness for males and females between 15–24 years of age as of 2003. Because of the difficulty in separating social phobia from poor social skills or shyness, some studies have a large range of prevalence. 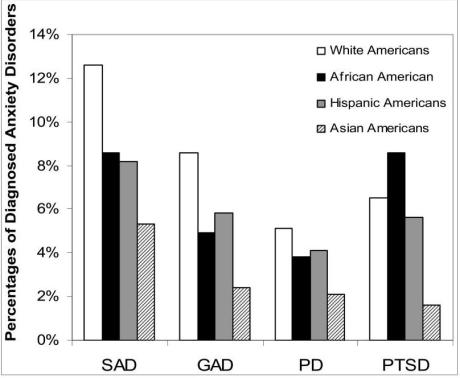
Prevention
The most important clinical point to emerge from studies of social anxiety disorder is the benefit of early diagnosis and treatment. Social anxiety disorder remains under-recognized in primary care practice, with patients often presenting for treatment only after the onset of complications such as clinical depression or substance abuse disorders.
Research has provided evidence for the efficacy of two forms of treatment available for social phobia: certain medications and a specific form of short-term psychotherapy called Cognitive-behavioral therapy (CBT), the central component being gradual exposure therapy.( prevention of syndromal and subsyndromal social anxiety , 2009 )
Psychotherapy
cognitive behavioral therapy (CBT) can be highly effective for several anxiety disorders, particularly specific phobias, panic disorder and social anxiety disorder.CBT, as its name suggests, has two main components, cognitive and behavioral. the cognitive component can help the patient question how they can be so sure that others are continually watching and harshly judging them. The behavioral component seeks to change people's reactions to anxiety-provoking situations. As such it serves as a logical extension of cognitive therapy, whereby people are shown proof in the real world that their dysfunctional thought processes are unrealistic. A key element of this component was gradual exposure, in which the patient was confronted by the things they fear in a structured, sensitive manner. Gradual exposure is an inherently unpleasant technique; and had high drop out rates. Ideally it involves exposure to a feared social situation that is anxiety provoking but bearable, for as long as possible, two to three times a week. The aim is to learn from acting differently and observing reactions. This is intended to be done with support and guidance, and when the therapist and patient feel they are ready. Cognitive-behavioral therapy for social phobia for few patients now includes anxiety management training, which may include techniques such as deep breathing and muscle relaxation exercises, which may be practiced 'in-situ'. These early interventions, for some, can be useful but for most can become safety seeking behaviors so need to be suggested in a considered case conceptualization. CBT can also be conducted partly in group sessions, facilitating the sharing of experiences, a sense of acceptance by others and undertaking behavioral challenges in a trusted environment. (J Am Acad Child Adolesc Psychiatry. 2007 Dec
Pharmacological treatments
Selective serotonin reuptake inhibitors (SSRIs), a class of antidepressants, are considered by many to be the first choice medication for generalized social phobia. These drugs elevate the level of the neurotransmitter serotonin, among other effects. The first SSRI formally approved by the Food and Drug Administration was paroxetine, sold as Paxil in the U.S. or Seroxat in the UK. It was also the first antidepressant of this class specifically approved to treat social anxiety disorder in both children and adults. Compared to older forms of medication, there is less risk of tolerability and drug dependency associated with SSRIs. However, their efficacy in treating anxiety disorders and increased suicide risk has been subject to controversy.SSRIs can actually increase anxiety in some people. While this increase may only be a start-up side effect that will go away in a few weeks, it can be severe enough to warrant discontinuing the medication or temporarily adding an anti-anxiety medication. (Facing the challenge of social anxiety disorder , 1999)
Other drugs
Anti-depressants such as monoamine oxidase inhibitors (MAOIs) were frequently used in the treatment of social anxiety. Their efficacy appears to be comparable or sometimes superior to SSRIs or benzodiazepines. However, because of the dietary restrictions required, high toxicity in overdose, and incompatibilities with other drugs, its usefulness as a treatment for social phobics is now limited. Some argue for their continued use, however, or that a special diet does not need to be strictly adhered to. A newer type of this medication, Reversible inhibitors of monoamine oxidase subtype A (RIMAs) such as the drug moclobemide, inhibit the MAO enzyme only temporarily, improving the adverse-effect profile. (Pharmacotherapy of social anxiety disorder , 2006)
Benzodiazepines such as clonazepam are an alternative to SSRIs. These drugs are often used for short-term relief of severe, disabling anxiety. Although benzodiazepines are still sometimes prescribed for long-term everyday use in some countries, there is some concern over the development of drug tolerance, dependency and misuse. It has been recommended that benzodiazepines are only considered for individuals who fail to respond to safer medications. Benzodiazepines augment the action of GABA, the major inhibitory neurotransmitter in the brain; effects usually begin to appear within minutes or hours. (Neurobiology and pharmacotherapy of social phobia ,2004)
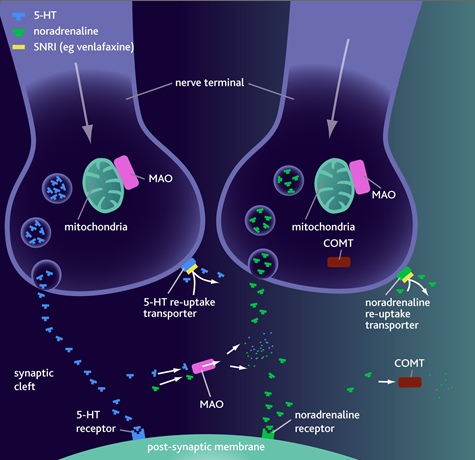
 Serotonin-norepinephrine reuptake inhibitors (SNRIs) such as venlafaxine have shown similar effectiveness to the SSRIs. In Japan, Milnacipran is used in the treatment of Taijin kyofusho a Japanese variant of social anxiety disorder.
Serotonin-norepinephrine reuptake inhibitors (SNRIs) such as venlafaxine have shown similar effectiveness to the SSRIs. In Japan, Milnacipran is used in the treatment of Taijin kyofusho a Japanese variant of social anxiety disorder.
The antidepressant mirtazapine has been proven effective in treatment of social anxiety disorder. This is especially significant due to mirtazapine's fast onset and lack of many unpleasant side-effects associated with SSRIs (particularly, sexual dysfunction). Another atypical antidepressant that has shown success is bupropion (Mirtazapine treatment of social phobia in women ,2005)
The combination of acute dosing of d-cycloserine (DCS) with exposure therapy facilitates the effects of exposure therapy of social phobia. DCS is an old antibiotic medication used for treating tuberculosis and does not have any anxiolytic properties per se. However, it acts as an agonist at the glutamatergic N-methyl-D-aspartate (NMDA) receptor site, which is important for learning and memory. It has been shown that administering a small dose acutely 1 hour before exposure therapy can facilitate extinction learning that occurs during therapy. (Augmentation Treatment of Psychotherapy for Anxiety Disorders with D-Cycloserine , 2006)