Eugenio Grillo e Caterina Franco
Introduction
The use of Proton Poumps Inibitors (PPI) like Omeprazole, can cause deficitary iron absorption which can lead to a reduction of the efficacy of Tryptophan as a niacin precursor.
This can cause the onset of a simil-Pellagra syndrome in patients with low intake, deficitary absorption or low production of nicotinic acid or nicotinamide (Vitamin B3)
Effect of proton pump inhibitors on vitamins and iron
PPIs may reduce the bioavailability of ingested vitamin C (Effect of proton pump inhibitors on vitamins and iron, 2009), that has a key role (The role of vitamin C in iron absorption, 1989) in iron absorption. Therefore proton pump inhibitors therapy reduces the absorption of non-heme iron. It may also retard clinical response to iron supplementation.
Iron deficiency reduces the endogenous synthesis of B3
Vitamin B3 can be synthetized from Tryptophan.
The metabolic pathway occurs through the formation of intermediates like N-formyl-kynurenine, kynurenine and quinolinate.
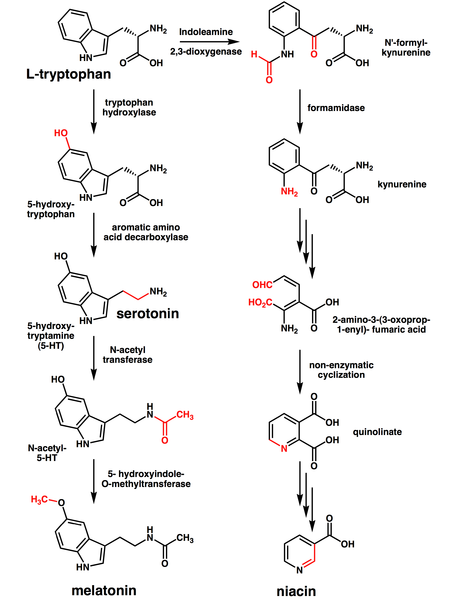
The conversion rate is about 60 mg of Trp for 1 mg of B3. Iron deficiency reduces the efficiency of this conversion (Iron deficiency reduces the efficacy of tryptophan as a niacin precursor, 1994).
That occurs because the first step is catalysed by Indoleamine 2,3-dyoxygenase (IDO-2,3) and Tryptophan 2,3-dyoxygenase (TDO-2,3) that are heme-containing oxygenases and so iron dependent enzymes (Density Functional Theory Study on a Missing Piece in Understanding of Heme Chemistry: The Reaction Mechanism for Indoleamine 2,3-Dioxygenase and Tryptophan 2,3-Dioxygenase, 2008).
Consequences of Vitamin B3 deficit
Vitamin B3 is a foundamental precursor of NAD. One recommended daily allowance of niacin is 2-12 mg/day for children, 14 mg/day for women, 16 mg/day for men and 18 mg/day for pregnant or breast-feeding women.
Niacin can be absorbed by the gut from its food sources or synthetized from tryptophan by the liver. The quote synthetized, although important, cannot supply an absence of dietary bioavaiable B3.
Population at risk is divided in three groups:
1. Insufficient of absent intake. Another possible cause of insufficient intake can be the low bioavaiability solved by the nixtamalization. This was the cause of the epidemic outbreak of Pellagra in the late 19th century.
2. Malabsorption.
3. Deficitary endogenous production. In patients with carcinoid syndrome a large amount of Trp is converted to Serotonin leaving a smaller amount available to be converted into niacin.
Chronic lack of Niacin commonly cause a vitamin deficiency disease called Pellagra
Pellagra is classically described by "the four D's": diarrhea, dermatitis, dementia and death. Mild niacin deficiency has also been shown to slow metabolism, causing decreased tolerance to cold. A more comprehensive list of symptoms includes:
- Aggression
- Dermatitis, alopecia, edema
- Weakness
- Mental confusion
- Ataxia, paralysis of extremities, peripheral neuritis
- Diarrhea
- Eventually dementia
Frostig and Spies (acc. to Cleary and Cleary) described more specific psychological symptoms of pellagra as:
- Psychosensory disturbances (impressions as being painful, annoying bright lights, odors intolerance causing nausea and vomiting, dizziness after sudden movements)
- Psychomotor disturbances (restlessness, tense and a desire to quarrel, increased preparedness for motor action)
- Emotional disturbances
Despite clinical symptoms, blood level of tryptophan or unrinary metabolites such as 2-pyridone/N-methylniacinamide ratio <2 or NAD/NADP ratio in erythrocytes could be used to diagnose pellagra. Diagnosis could be confirmed after rapid improvements in the symptoms in patients using high doses of niacin (50-500 mg/day) or niacin enriched food.
PPIs also reduce directly human niacin intake
Niacin intake in human gut although not well understood is highly dependent on extracellular acidic pH (Mechanism and regulation of human intestinal niacin uptake, 2005). Therefore PPIs, inhibiting the acidification of the stomach, directly inhibit B3 absorption.
Nicotinic acid prevents iron deficiency
Nicotinic acid, in addition to its known effect on growth and metabolism, may be playing an important role in enhancing zinc and iron utilization (Effect of nicotinic acid on zinc and iron metabolism, 1997). In animal experiments, when mice were fed with nicotinic acid-deficient, -adequate and -excess synthetic diets for four weeks it was observed that, in comparison with the nicotinic acid-deficient diet, percent zinc absorption, intestinal zinc, percent haeomoglobin and liver iron increased significantly under nicotinic acid-adequate and -excess conditions.
Effects of NAD/NADP deficiency
As previously said, Vitamin B3 is a foundamental precursor for the cofactors Nicotinamide Adenine Dinucleotide and Nicotinamide Adenine Dinucleotide Phosphate.
NAD
NAD has various essential roles in metabolism:
1. Cofactor in redox reactions
2. Donor of ADP-ribose moieties in ADP-ribosylation reactions
3. Precursor of the second messenger molecule cyclic ADP-ribose
4. As Adenine Dinucleotide, it has important extracellular roles (Release of beta-nicotinamide adenine dinucleotide upon stimulation of postganglionic nerve terminals in blood vessels and urinary bladder, 2004)
These roles are involved in energy metabolism, mitochondrial functions, calcium homeostasis, generation of oxidative stress, gene expression, immunological functions, aging, and cell death (NAD+/NADH and NADP+/NADPH in cellular functions and cell death: regulation and biological consequences, 2008).
NAD is also related to bone marrow's health and cancer progression (Niacin deficiency decreases bone marrow poly(ADP-ribose) and the latency of ethylnitrosourea-induced carcinogenesis in rats, 2002), and has a benefical role in preventing neurological degeneration (Nicotinic acid, nicotinamide, and nicotinamide riboside: a molecular evaluation of NAD+ precursor vitamins in human nutrition, 2008).
NAD and Niacin deficiency induce the enzyme Nicotinamide-N-Methyltransferase. High activity of this enzyme is related to Parkinson's Disease and cancer (Nicotinamide, NAD(H), and Methyl-Group Homeostasis Evolved and Became a Determinant of Ageing Diseases: Hypotheses and Lessons from Pellagra).
NAD, and mostly NAM (Nicotinamide), have a particular role in regulation of mesenchimal stem cells. NAM is converted in NAD by the enzyme Nicotinamide phosphoribosyltransferase (Nampt). The activity of this enzyme determines the NAD/NAM ratio.
A good NAD supply increases bone mineralization and stimulates osteocyte proliferation.
A bad NAD supply, represented by an high concentration of NAM, induces adipocyte proliferation and blocks osteocyte growth, potentially leading to osteoporosis (Nicotinamide phosphoribosyltransferase (Nampt) affects the lineage fate determination of mesenchymal stem cells: a possible cause for reduced osteogenesis and increased adipogenesis in older individuals, 2011)
A NAD deficiency can then cause:
1. Deceleration of glycoliosis, Kreb's cycle and most of all electron transport chain
2. An increased susceptibility to ROS damage
3. Bone marrow and brain sufference
4. An increased adipocyte proliferation
5. An increased risk of osteoporosis
NADP
NADP has various roles in metabolism:
1. Coenzyme in anabolic reactions
2. Regenerator of reduced glutathione (GSH)
3. Source of reducing equivalents for Cytocrome P450 hydroxilations
NADP deficiency leads to higher sensibility to oxydative damage (NAD+/NADH and NADP+/NADPH in cellular functions and cell death: regulation and biological consequences, 2008), and higher sensibility to the toxic substrates of Cytocrome P450 (about 75% of drugs, ethanol).