The botulinum toxin is a proteic neurotoxin produced by the Clostridium botulinum.
Clostridium bacterium
The Clostridium bacterium is an obligate anaerobic (it lives only in absence of Oxygen because it doesn’t have a cytochromes system and it is forced to produce ATP using the fermentation of different substrates ), GRAM positive, spore-former bacterium. Clostridii are usually found in the upper part of soil and are responsible of human affections only after an accidentally introduction of the bacterium because of a wound or after the ingestion of aliments infected by the toxin.
Toxin
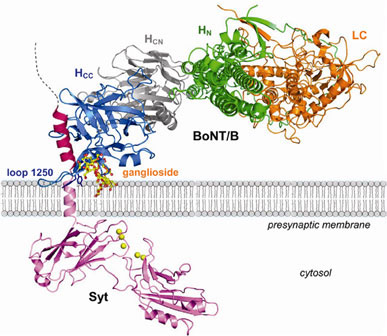
The botulinum toxin is a polypeptide made by 2 chains joined by a disulfide bond; the first subunit is the heavy chain (100kDa), it is also called “H-chain” because it is the one who bonds with the receptors of the target neurons and activates the endocytosis of the second chain (the light chain, 50kDa, also called L-chain). Once arrived in the cytoplasm the L-chain attacks one of the fusion proteins (SNAP-25, Syntaxin or Synaptobrevin, that are part of the SNAREs proteins family) at a neuromuscolar junction, preventing vesicles from anchoring to the membrane to release acetylcholine, in order to interfere with the nerve impulses and causing flaccid paralysis of muscles.

We know seven different types of botulinum toxin, designated A through G and produced by seven types of Clostridium botulinum. A, B and E types are the main responsibles for human poisoning. Once ingested, the toxin arrives in the intestine without being inactivated by the proteolytic enzymes, it is absorbed and it starts to be spread through the blood. It arrives at the neuromuscolar junction and to all the cholinergic pre and post-ganglia nerve endings of the PNS.
Botulism
The botulinus intoxication or Botulism is a rare but sometimes fatal paralytic illness caused by botulinum toxin.
Foodborne botulism can be transmitted through food that has not been heated correctly prior being canned; it usually results from ingestion of food that has become contaminated with spores in an anaerobic environment, which allows the growth of the bacteria that produces toxin. It’s the ingestion of the toxin that causes botulism, not the ingestion of the spores or the vegetative bacteria. Once the toxin has been ingested it is coiled by a wrap made by proteins which keep it protected from the gastric acid pH. When the toxin arrives in the bowel the alkaline pH destroys the proteinaceous wrap and so the toxin can be absorbed and spread through blood and lymph. Proper refrigeration below 3°C retards the growth of Clostridium botulinum; the organism is also susceptible to high salt, high oxygen and low pH level. The toxin itself is rapidly destroyed by heat (for example cooking process), meanwhile the spores that produce the toxin are heat-tolerant and will survive boiling water for an extended period of time.
Infant and wound botulism both result from infection with spores, which subsequently germinate, resulting in production of toxin and the symptoms of botulism.
Botulism can result in death due to respiratory failure, caused by the paralysis of the respiratory muscles, so treatment consists of antitoxin administration and artificial ventilation until the neurotoxin are excreted or metabolised. Patients with severe botulism may require intensive medical and nursing care for several months, and even after they survive they may have fatigue and shortness of breath for years, and long-term therapy may be needed to aid their recovery.
There are two primary botulinum antitoxins available:
- Trivalent (A, B, E), derived from equine sources using whole antibodies.
- Heptavalent (A, B, C, D, E, F, G), derived from equine sources using despeciated IgG antibodies, which have had the Fc portion cleaved off.
Several clinic uses of the toxin
In late 1970s, Alan Scott, an American ophtalmologist, and Edward Shantz were the first to work on a standardized botulinum toxin preparation for therpeutic purposes. After several experiments on monkeys, Scott used BTX-A for the first time in humans to treat “crossed eyes”(strabismus) and “uncontrollable blinking” (blepharospasm) by injecting overactive muscles with minute quantities of botulinum toxin type-A. This decreased the muscle activity by blocking the release of acetylcholine from the neuron by preventing the vesicle where the acetylcholine is stored from binding to the membrane where the neurotransmitter can be released. This effectively weaken the muscle for a period of three to four months.

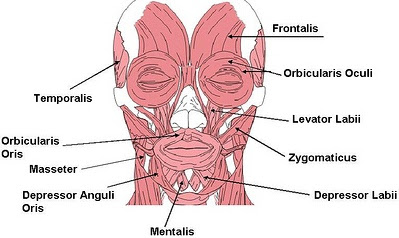
The BTX-A is now available in freeze-dried form for injection that are useful to treat spasms and dystonias but also have a cosmetic application; in fact Botox is used to prevent development of wrinkles by paralyzing facial muscles or to temporarily improve the appearence of moderate-to-severe frown lines between the eyebrows.
In the USA, Botox is manufactured by Allergan, Inc, Xeomin is manufactured in Germany by Merz and Dysport is manufactured in Ireland. The last one is for therapeutic use only, while the other 2 are available for both therapeutic and cosmetic use.
The BTX-B (used to treat cervical dystonia) is sold in Europe with the name of Neurobloc.
Major illness treated with BTX-A
Hemifacial Spasm is a rare neuromuscular disease characterized by irregular, involuntary muscle contractions on just one side of the face. HFS can start with the intermittent twitching of the eyelid, which can result in forced closure of the eye. The spasm usually starts from the forehead or from the lower part of the face, but sometimes it can involve the superficial muscles of the front side of the neck. This disease is often unaffected and it seldom comes from a facial trauma, there are also some causes that can make it worse like bright lights, stress and intense emotions.
The main cause of HFS is the pulse of a blood-vessel located in the point in which the facial nerve comes out of brainstem. The facial nerve controls muscles that influence facial expressions, its contact with the blood vessel irritates it causing the spasm.

The pharmacological oral treatment isn’t really effective, for this reason the main treatment are botulinum injections; the injection is made directly in the muscle that present spasms or in the subcutis. The toxin relax the muscle by partially paralyzing it causing the reduction or the disappearance of the spasms. Anyway the effect is only temporary (3 through 6 months) and the treatment needs to be repeated once it is expired.
Blepharospasm is any abnormal contraction or twitch of the eyelid, it normally refers to benign essential blepharospasm, a focal dystonia (a neurological movement disorder involving involuntary and sustained contractions of the muscles around the eyes). The patient’s eyelids feel like they are clamping shut and will not open without great effort.
Patients don’t usually have ocular ilnesses, but for periods of time they are effectively blind due to their inability to open their eyelids, they are also very sensitive to bright lights and may have issues from the dryness of the eyes. Sometimes symptoms radiate into the nose, face and the neck area.
Drug therapy has proved generally unpredictable and short-termed. The treatment used in this case are Botulinum toxin injection, in order to induce localized, partial paralysis. These injections are generally administered every three months, with variations based on patient response and usually give immediate relief of symptoms from the muscle spasm.
Distonya is a neurological movement disorder, in which sustained muscle contractions cause twisting and repetitive movements or abnormal postures due to the fact that there is the double implications of agonist and antagonist muscle. This disease is suspected to be caused by a pathology of the central nervous system, likely originating in those parts of the brain concerned with motor function, such as the basal ganglia, but the physiopatolocig causes are still unknown.
- Oromandibular dystonia is a form of local dystonia affecting the mouth (opening/closing movements), jaw and tongue and in this decease it is hard to speak.
Studies made by ENT Department of James Cook University Hospital in Middlesbrough, UK has shown that patients affected by this particular type of dystonia treated with BTX-A injections actually felt improvements and this can be also proved by The Oromandibular Dystonia Questionnaire that is the first reliable and valid instrument to measure health-related quality of life in patients with oromandibular dystonia.
[“Oromandibular dystonia questionnaire (OMDQ-25): a valid and reliable instrument for measuring health-related quality of life.” Clin Otolaryngol. 2010 Oct, PubMed]
- Meige Syndrome is a type of Dystonia, actually a combination of two forms of dystonia: Blepharospasm and Oromandibular dystonia. It is characterised by bilateral involuntary activity of facial and perioral muscles combined with blepharospasm.
A case of a 15-year-old boy with Meige syndrome was treated with injection of botulinum toxin and the results were collected by the Maxilo-Facial Unit of the Provincial General Hospital in Badulla, Sri Lanka. They showed successful exits.
[“Meige syndrome: a rare form of cranial dystonia that was treated successfully with botulinum toxin.” Br J Oral Maxillofac Surg. 2008 Oct, PubMed]
- Cervical Dystonia or Spasmodic Torticollis is an extremely painful chronic neurological movement disorder causing the neck to involuntarily turn to the left, right, upwards, and/or downwards. Both agonist and antagonist muscles contract simultaneously during dystonic movement. This disease is cured with Botulinum toxin type B, (which has been approved by FDA, drugs like Myobloc in the USA and Neurobloc in European Union). The study made by Department of Neurology of St. George’s hospital of London, UK showed how the treatment has been improved under the guidance of EMG, that proved a laterocervical approach better than any other because in this way (by injecting the toxin on the longus colli or in addition on the sterno-cleido-mastoideo muscles) they could avoid dysphagia, an additional side effect detected in patient with ‘goose-neck’ or ‘double-chin’ posture.
[“Anterior and posterior sagittal shift in cervical dystonia: a clinical and electromyographic study, including a new EMG approach of the longus colli muscle.” Mov Disord.2011 Nov, PubMed]

Bruxism is an oral parafunctional activity, it is an excessive grinding of the theet or excessive clenching of the jaw that can occur when the patient is asleep or awake. This distinction needs to be done since the two manifestations have different causes: awake bruxism is thought to be usually semivoluntary, and often associated with stress caused by family responsibilities or work pressures while sleep bruxism is caused by mechanisms related to the central nervous system, involving sleep arousal and neurotransmitter abnormalities. Botox has been suggested as a treatment for this disease, there is only one randomized control trial which has reported that Botox reduces the myofascial pain symptoms. Botox injections are used on the theory that a dilute solution of the toxin will partially paralyze the muscles and lessen their ability to forcefully clench the jaw without avoiding normal activities such as talking and eating. This treatment typically involves five or six injections into the masseter and termporalis muscles, and less often into the lateral pterygoids (given the possible risk of decreasing the ability to swallow). It takes a few minutes per side, and the patient may start feeling the effects by the next day, and may last for about three months. Occasionally, adverse effects may occur, such as bruising, but this is quite rare.
Spasticity is a feature of altered skeletal muscles performance in muscle tone involving hypertonia spasticity, clinically is defined as velocity dependent resistance to stretch. It mostly occurs in disorders of the central nervous system (CNS) impacting the upper motor neuron in the form of a lesion, such as spastic diplegia, but it can also present in various types of multiple sclerosis. In some case Botulinum toxin injections are used into the muscle belly, to attempt to dampen the signals between nerve and muscle.
Side Effects
During treatments with Botox patients sometimes show some adverse reactions; side effects are rare and consist in the possible paralysis of the wrong muscle group and allergic reaction. Bruising at the site of injection is a side effect not of the toxin, but rather the mode of administration. In cosmetic use, this can result in inappropriate facial expression, such as drooping eyelid, double vision, uneven smile, or loss of the ability to close eyes. This will wear off in around six weeks. Bruising is prevented by the clinician applying pressure to the injection site, but may still occur, and will last around seven to 11 days. When injecting the masseter muscle of the jaw, loss of muscle function will result in a loss or reduction of power to chew solid foods.
Moreover Botox has been linked in cases of respiratory failure and death, due to its ability to spread to areas distant from the site of the injection; however this represents an exigue possibility since the minimum dose of toxin used for medical purposes does not imply the development of botulism.
Conclusions
All of what we have written shows up that in spite of the lethal and terrible effects that Botulinum toxin brings, modern medicine managed to find its way in making it useful, effective and able to improve the life quality of millions of people.
Bibliography
2008, La Placa & Co. “Principi di Microbiologia Medica” – Undicesima Edizione. Ed. Società Editrice Esculapio – Bologna, Italy
2009, Harrison & Co. “Principi di Medicina Interna” – Diciassettesima Edizione. Mc Graw Hill Ed. - CTPS, Hong Kong, China
Webography
http://en.wikipedia.org/wiki/Hemifacial_spasm. - “Hemifacial spasm”, Wikipedia
http://en.wikipedia.org/wiki/Botulinum_toxin. - “Botulinum toxin”, Wikipedia
http://en.wikipedia.org/wiki/Blepharospasm. - “Blepharospasm”, Wikipedia
http://en.wikipedia.org/wiki/Meige_syndrome. - “Blepharospasm”, Wikipedia