Obesity Overview
Obesity Pathway
As we were....(1952)

The role of environment and diet

Temperature
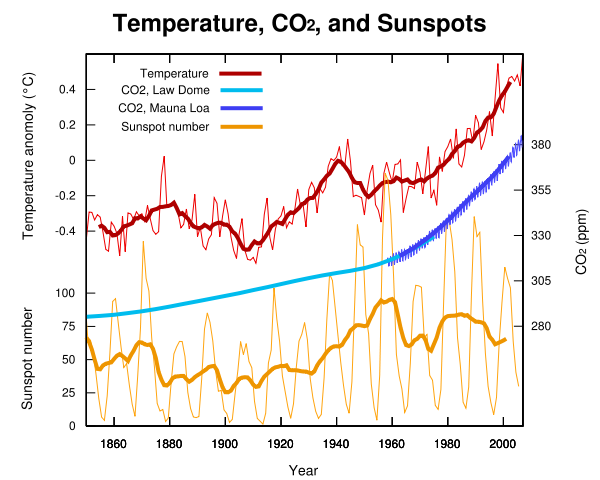
T anomaly 1880-2005

CO2
Inflammation
Overweight children have higher circulating hepcidin concentrations and lower iron status but have dietary iron intakes and bioavailability comparable with normal weight children 2009
Food Intake: aggregated and disaggregated
Calcio e vitamina D prevengono aumento di peso
L'integrazione di calcio e vitamina D ha un lieve effetto preventivo sull'aumento di peso nelle donne in età postmenopausale, e soprattutto in quelle con un'assunzione di calcio inadeguata. L'obesità si è diffusa significativamente negli ultimi decenni, ed il ruolo del calcio nel mantenimento di un peso sano rimane controverso. La prevenzione dell'aumento di peso è un importante traguardo a livello di salute pubblica, e la restrizione calorica e l'attività fisica quotidiana dovrebbero ancora essere considerate le basi della gestione del peso: sono necessarie ulteriori ricerche sulla combinazione del calcio con queste due strategie per la prevenzione dell'aumento di peso, e nel frattempo alle donne in età postmenopausale dovrebbe ancora essere consigliata l'assunzione di 1200 mg di calcio al giorno. (Arch Intern Med. 2007; 167: 893-902)
BMI eccessivo aumenta mortalitÃ
Un BMI al di sopra del range ideale potrebbe causare un ampio incremento nei tassi di mortalità . Le principali associazioni fra BMI e mortalità complessiva e specifica possono essere valutate al meglio dall'osservazione prospettica a lungo termine di campioni molto abbondanti. Benchè altri parametri antropometrici come la circonferenza della vita ed il rapporto vita-anca potrebbero aggiungere informazioni significative al BMI, già il BMI in sé stesso è un forte fattore predittivo di mortalità sia al di sopra che al di sotto dei 22,5-25 Kg/m2. L'aumento progressivo di mortalità al di sopra di questo intervallo è dovuto principalmente a malattie vascolari. Con 30-35 kg/m2 la sopravvivenza media si riduce di due-quattro anni, e con 40-45 kg/m2 si riduce di otto-dieci anni, il che è paragonabile all'effetto del fumo. Al di sotto dei 22,5 kg/m2 l'aumento di mortalità si deve eminentemente a malattie collegate al fumo, e non è stato pienamente spiegato. In età adulta potrebbe risultare più semplice evitare sostanziali aumenti di peso che perderne una volta che è stato accumulato. Evitando un ulteriore aumento da 28 a 32 kg/m2, un tipico soggetto di mezza età guadagnerebbe circa due anni di speranza di vita, che diverrebbero tre in un soggetto giovane che evita di passare da 24 a 32 kh/m2. (Lancet online 2009, pubblicato il 18/3)
Acylation stimulating protein is associated with pregnancy weight gain. 2008
Endocrinologia
Gravi rischi per le anziane in sovrappeso
Aumentare di peso nel corso degli anni e risultare in sovrappeso in età avanzata comprometterebbe in maniera molto seria la salute delle donne. Valutazioni dettagliate riguardanti incidenza di patologie croniche, funzioni fisiologiche e capacità cognitive in donne settantenni hanno permesso di stabilire una chiara correlazione tra stato di salute e peso corporeo. In particolare, gli autori dell'indagine pubblicata su British Medical Journal, seguendo la storia clinica di oltre 17mila donne, a partire dall'età di 50 anni, hanno potuto osservare un decremento della qualità della vita direttamente legato all'aumento di peso corporeo. Partecipanti con indice di massa corporea maggiore di 30 hanno mostrato probabilità inferiori al 79% di vivere senza malattie croniche, quali cancro e patologie cardiovascolari, rispetto a donne con indice compreso tra 18,5 e 22,9. «Quanti più chili la donna prende nel periodo compreso tra i 18 anni e la mezza età tanto più elevato diventa il rischio di deteriora
Appetite. 2009 Jun;52(3):675-83. Epub 2009 Mar 20.
Alpha1- and alpha2-containing GABAA receptor modulation is not necessary for benzodiazepine-induced hyperphagia.
Morris HV, Nilsson S, Dixon CI, Stephens DN, Clifton PG.
Department of Psychology, University of Sussex, Falmer, Brighton, UK.
Benzodiazepines increase food intake, an effect attributed to their ability to enhance palatability. We investigated which GABA receptor subtypes may be involved in mediating benzodiazepine-induced hyperphagia. The role of the alpha2 subtype was investigated by observing the effects of midazolam, on the behavioural satiety sequence in mice with targeted deletion of the alpha2 gene (alpha2 knockout). Midazolam (0.125, 0.25 and 0.5mg/kg) increased food intake and the amount of time spent feeding in alpha2 knockout mice, suggesting that BZ-induced hyperphagia does not involve alpha2-containing GABA receptors. We further investigated the roles of alpha1- and alpha3-containing GABA receptors in mediating BZ-induced hyperphagia. We treated alpha2(H101R) mice, in which alpha2-containing receptors are rendered benzodiazepine insensitive, with L-838417, a compound which acts as a partial agonist at alpha2-, alpha3- and alpha5-receptors but is inactive at alpha1-containing receptors. L-838417 (10 and 30 mg/kg) increased food intake and the time spent feeding in both wildtype and alpha2(H101R) mice, demonstrating that benzodiazepine-induced hyperphagia does not require alpha1- and alpha2-containing GABA receptors. These observations, together with evidence against the involvement of alpha5-containing GABA receptors, suggest that alpha3-containing receptors mediate BZ-induced hyperphagia in the mouse.
Naltrexone/bupropione combinazione anti-obesità
Una combinazione a rilascio sostenuto di naltrexone più buproprione potrebbe rivelarsi un'utile opzione terapeutica per il trattamento dell'obesità. Lo suggerisce lo studio randomizzato, in doppio cieco, placebo controllato di fase 3 Contrave obesity research I (Cor-I), condotto da Frank Greenway del Louisiana State University System di Baton Rouge (Stati Uniti), e collaboratori, su 1.742 soggetti di età compresa tra 18 e 65 anni: i partecipanti avevano un indice di massa corporea (Bmi) di 30-45 Kg/m2 e obesità non complicata oppure un Bmi di 27-45 Kg/m2 con dislipidemia o ipertensione. Ai pazienti sono stati prescritti una leggera dieta ipocalorica ed esercizio fisico e si è proceduto alla randomizzazione in tre gruppi: naltrexone a rilascio sostenuto 32 mg al giorno più bupropione a rilascio sostenuto 360 mg al giorno combinati in tavolette a dosi fisse; naltrexone a rilascio sostenuto 16 mg al giorno più bupropione a rilascio sostenuto 360 mg al giorno combinati in tavolette a dosi fisse; placebo 2 volte al giorno. Il trattamento è proseguito per 56 settimane in 870 pazienti. La variazione media del peso corporeo è risultata pari a -1,3% nel gruppo placebo, a -6,1% nel gruppo naltrexone 32 mg più bupropione e -5,0% nel gruppo naltrexone 16 mg più bupropione. 84 partecipanti (16%) del gruppo placebo hanno beneficiato di una riduzione del peso corporeo del 5% o superiore rispetto ai 226 pazienti (48%) assegnati al gruppo naltrexone 32 mg più bupropione e ai 186 pazienti (39%) del gruppo naltrexone 16 mg più bupropione. Il più frequente evento avverso nei gruppi assegnati al trattamento di combinazione era la nausea (29,8% nel gruppo naltrexone 32 mg e 27,2% nel gruppo naltrexone 16 mg vs 5,3% del gruppo placebo). La terapia con naltrexone e bupropione ha anche comportato una maggiore frequenza di mal di testa, costipazione, vertigini, vomito e secchezza delle fauci. Nel gruppo trattato con i due farmaci si è osservato un incremento transitorio di circa 1,5 mmHg della pressione arteriosa sistolica e diastolica seguito da una riduzione di circa 1 mmHg al di sotto del valore basale. Rispetto al placebo la terapia di combinazione non è risultata associata ad un aumento della depressione e di eventi suicidari
The Lancet 2010; 376: 595-605
"Mike Geary and flat":