Introduction
Sugars consumption has increased worldwide, especially in America, paralleling the epidemic of obesity. Because of the increasingly widespread use of sweeteners such as sucrose and HFCS, the American diet is the richest in the world of cereals extracted fructose. This article will explore it recent history and its role in energy homeostasis.
In order to distinguish the natural fructose from the cereal extracted fructose, even if the fructose molecule is the same, I will refer for simplicity to both of them with the term of “fructoses”.
Consumption of high-fructose corn syrup in beverages may play a role in the epidemic of obesity. 2004
Fructose, weight gain, and the insulin resistance syndrome, 2002

History, consumption and industrial use
Fructose, or fruit sugar, is a simple monosaccharide found in many plants, where it is often bonded to glucose to form the disaccharide sucrose. It is one of the three dietary monosaccharaides, along with glucose and galactose, which are absorbed directly into the bloodstream during digestion.
Fructose
Because since the 70s the demand for sugar has globally increased, the food industry has been producing low-cost artificial sugars rich in fructose extracting them from cereals, encouraged by the high price of sucrose and the low price of corn.
In fact, in the 70s the American mean daily per capita consumption of fructoses was estimated to be 37 g / day, accounting for 8% of the daily calories requirements. In a study of 2008 consumption was calculated to be 54.7 g / day (range 38.4-72.8), account for 10.2% up to 15% of daily energy intake. The data show that the prevalence of obesity in the U.S. population has increased over the same time period as the increase in fructoses consumption: now it is estimated that over 10% of Americans' daily calories are from fructoses.
This is principally due to an increase in the use of sweeteners in foods and beverages.
The most common sweeteners are sucrose and high fructose corn syrup (HFCS), two substances with similar composition: 50% fructose and 50% glucose in sucrose, about the same in HFCS. HFCS is a liquid sweetener used in the manufacturing of foods and beverages, with a particularly interesting history. The difference between the two, is that the first (sucrose) is a disaccharide naturally present in sugar cane or beet, while the second is an artificial mixture of two oligosaccharides resulting from an industrial extraction process of transformation of corn, which includes the use of enzymes.

A relevant fact is that while sucrose consumption, from the 70s, has decreased by almost the 50%, that of fructoses has increased by 1000%, from about 250g / year to about 25 kg / year. The industrial production process of HFCS was invented by Yoshiyuki Takasaki and consists of a series of steps:
- the corn is ground in mills obtaining corn starch.
- than it’s converted into corn syrup, which consists almost entirely in dextrose
- at this point are added enzymes that isomerize part of the dextrose to produce a 42% fructose syrup called HFCS-42.
- By passing HFCS-42 through an ion-exchange column that retains fructose, corn refiners draw off 90-percent HFCS and blend it with HFCS-42 to make a third syrup, HFCS-55. This latter is the most used type of HFCS in the food industry, about 60%.
Dietary fructose consumption among US children and adults-the third national health and nutrition examination survey, 2004
Fructose, weight gain, and the insulin resistance syndrome, 2002
USDA ERS – Sugar & Sweeteners: Background
High Fructose Corn Syrup

Sources of fructoses
The most important sources of fructoses in a typical American diet are, about on average:
- 30,1% sweetened beverages
- 21,5% grains, which includes processed food such as cakes, pies and snacks as well as breads and cereals
- 19,4% fruit or fruit juices
- 10,8% sweets
- fresh cheeses, creams, dressing sauces
- ham, sausages, wurstels
High-fructoses diet are common especially in the age group between 12 and 30 years; the picture below shows the sources of fructoses to a band of the American population between 12 and 18 years.
Dietary fructose consumption among US children and adults: the third national health and nutrition examination survey, 2004

Fructoses' Metabolism
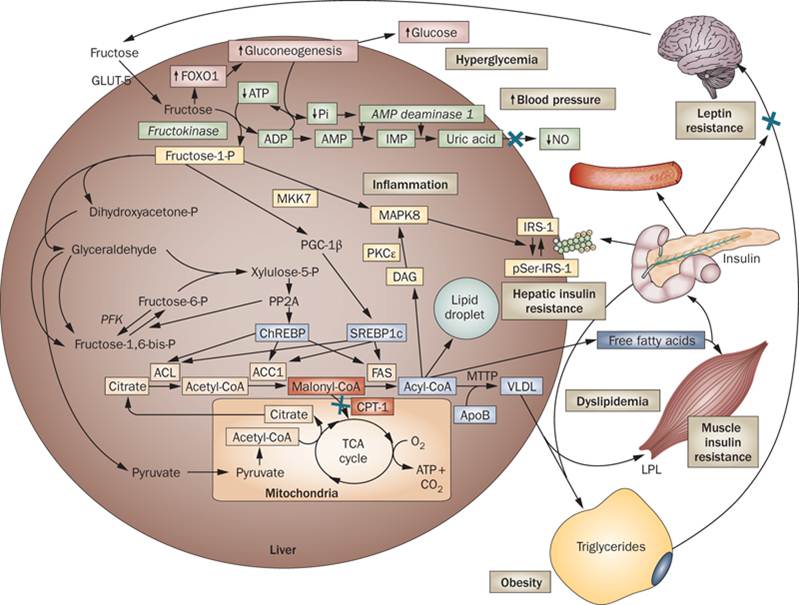
Hepatic metabolism
Fructoses are not distributed to the various cells of the body but are metabolized only by the liver, and their hepatic metabolism has a significant effect on both glucose and lipid metabolism at the same time.
Only the liver possesses the GLUT5 transporter, and indeed has a very high fructose extraction rate. Fructose is phosphorylated independently of insulin to fructose-1-phosphate by the enzyme fructokinase. So, bypassing the main stage in the control of glycolysis catalysed by phosphofructokinase, fructose-1-phosphate undergoes glycolysis; than the aldolase-B splits it into glyceraldehyde and dihydroxyacetone-phosphate, that consequently will be metabolised to pyruvate.
This leads to a greater activity of the enzyme pyruvate dehydrogenase and the enzyme lactate dehydrogenase, and the result is:
- large volume of acetyl-CoA entering the mitochondrial tricarboxylic acid cycle. Any extra intermediary will be available for de novo liponeogenesis (DNL)
- an increased concentration of citrate and ATP, that inhibit phosphofructokinase
- an increased concentration of lactate
Effects on insulin secretion
Only marginally insulin secretion is stimulated by fructoses, which means that in response to a high fructoses load, insulin levels vary little. This is due to two main reasons:
- low expression of GLUT 5 (glucose transporter 5) in beta-cells of the pancreas
- blood-brain barrier (BBB) is impermeable to fructose. This involves that fructose molecule can’t trigger the central nervous system (CNS) glucose sensors responsible for the food intake regulation.
Fructose: it’s alcohol without the buzz, 2013
Intermediary Metabolism of fructose, 1993
Fructoses and energy balance
With meals high in fructoses, the most significant implications for energy homeostasis are:
1. Decreasing sensation of satiety and increasing caloric consumption. Fructose molecule, unlike glucose, does not stimulate the production of insulin (which in turn is responsible for the release of leptin from adipocytes) and does not inhibit the one of ghrelin. The consequence in the ventral hypothalamus, where there are the principal regulatory centers of energy homeostasis, are opposite to those of glucose: the hunger centers (laterally) continue to be stimulated by ghrelin, while satiety centers (medially) are not inhibited for the lack of leptin and insuline.
So fructose molecule is "invisible" to CNS energy homeostasis centers, and then behaves as a source of "empty calories" that go unnoticed.
Although those results are very clear in animals consuming high-fructoses diet, considerably less information is available about humans. However, in the few studies conducted on human subjects who consumed large amounts of sucrose or soda sweetened with HFCS (high-fructose diets) was shown an increase in energy intake, body weight, fat mass, hyperphagia and blood pressure. In these studies of fructoses or sucrose feeding in humans, the subject did not compensate for the energy consumed as fructoses by reducing ad libitum energy intake from other sources.
Consumption of high-fructose corn syrup in beverages may play a role in the epidemic of obesity, 2004
Dietary fructose consumption among US children and adults: the third national health and nutrition examination survey, 2004
2. Increased de novo lipogenesis (DNL): Any extra acetil-CoA not entering in the Krebs Cycle will be available for de novo lipogenesis (DNL), and then for the conversion into triglycerides (TG), which lead to:
- storation in hepatocytes with the risk of: steatosis, non-alcoholic steatohepatitis, cirrhosis
- the levels of plasma triglycerides increase, both free (NEFA ad FFA) and included in lipoprotein. There is an increase in releasing VLDL from the liver, which is accompanied by a decrease in HDL blood levels and an increased conversion of VLDL to LDL. The data of a 1995 study, involving the collaboration of Gerald Reaven and Jorgen Jeppesen, show that both oral fat or fructose loads accentuate the degree of postprandial lipemia. More than ten years before Gerald Reaven demonstrated that feeding healthy people with a diet containing 60% carbohydrates (too many) give as result an increase of triglycerides and VLDL to LDL, while HDL lipoproteins are reduced.
This has long-term consequences such as:
- increased abdominal obesity
- increased risk of atherogenesis, which is reflected in cardiovascular diseases such as myocardial infarction (MI), atherosclerosis, coronary artery disease (CAD), hypertension. A good marker of risk for these kind of diseases is the TG/HDL ratio greater than 3
(TG/HDL > 3)
Gusto e Salute, Beppe Rocca, 2013
Fasting triglycerides, high-density lipoprotein, and risk of myocardial infarction, 1997
Effect of variations in oral fat and carbohydrate load on postprandial lipemia, 1995
Plasma glucose, insulin and lipid responses to high-carbohydrate low-fat diets in normal humans, 1983
3. Contribution to insulin resistance: Even if fructose molecule does not stimulate insulin secretion in the short term, a long-term fructoses feeding induces insulin resistance which means a paradoxical compensatory hyperinsulinemia. The two main causes are:
- high levels of cytoplasmic fructose-1-phosphate activate the inflammatory cascade leading to the activation of the transcription factor MAPK8, which phosphorylates the serine of the insulin receptor IRS-8 which undergoes functional inactivation.
- By increasing the hepatic and beta-cells intracellular lipid content, that first of all destabilize membranes by altering their lipid concentration and leading to misfolding of its transmembrane proteins and receptors
Fructose, weight gain, and the insulin resistance syndrome, 2002
Beppe Rocca, Gusto e Salute, 2013
Other effects of excessive amounts of fructoses in the diet (which I will not deal here in detail) are:
- contribution to insulin hyperglycemia, because fructose activate the transcription factor FOX01 which is a positive regulator of gluconeogenesis
- contribution to gout and hyperuricemia
- contribution to increased blood pressure by the reduction of NO, a consequence of higher plasma levels of uric acid
- increased of type 2 diabetes risk by the exaggerated production of AGE (Advanced Glycation End--products)
Conclusions: another piece of the puzzle
Diets high in fructoses are harmful to health, and certainly predispose the subject to a fertile context for obesity and metabolic syndrome, reason why we must not exceed their consumption. A good start would be to begin decreasing the consumption of sweetened beverages and processed food.
For example, in European Community countries, in which the consumption of HFCS is currently limited to about 5% of food total sugar, the percentage of obese population is much lower than in America.
Fructoses, however, are just another piece of the puzzle of these complex, multifactorial and environmentally chronic diseases, and demonizing them the problem will be not solved.
