Hashimoto's thyroiditis or chronic lymphocytic thyroiditis is believed to be the most common cause of primary hypothyroidism. It occurs far more often in women than in men (10:1 to 20:1), and is most prevalent between 45 and 65 years of age.
Also known as Hashimoto's disease, Hashimoto's thyroiditis is named after the Japanese physician Hashimoto Hakaru (1881−1934) of the medical school at Kyushu University, who first described the symptoms in 1912 in a German publication.
Hashimoto's Thyroiditis is a type of autoimmune thyroid disease which the immune system attacks and destroys the thyroid gland . The thyroid helps set the rate of metabolism, which is the rate at which the body uses energy. Hashimoto’s stops the gland from making enough thyroid hormones for the body to work the way it should. It is the most common thyroid disease in the U.S.

EPIDEMIOLOGY
United States
Hashimoto thyroiditis is the most common cause of hypothyroidism in the United States after the age of 6 years, with incidence estimated to be 1.3% in a series of 5000 children aged 11-18 years. In adults, incidence is estimated to be 3.5 per 1000 per year in women and 0.8 per 1000 per year in men. Incidence may be as high as 6% in the Appalachian region. In the Colorado Thyroid Disease Prevalence Study involving 25,862 adults, the prevalence of elevated TSH in both symptomatic and asymptomatic adults was 9.5%, with a greater percentage of those involved being women. The prevalence of hypothyroidism and thyroid disease in general increases with age.

International
Worldwide, the most common cause of hypothyroidism is iodine deficiency However, Hashimoto thyroiditis remains the most common cause of spontaneous hypothyroidism in areas of adequate iodine intake.
The incidence of Hashimoto thyroiditis worldwide is estimated to be 0.3-1.5 cases per 1000 of population per year. Tunbridge et al in a study of 2779 patients in Whickham, England, found an incidence of 14 cases per 1000 females and less than 1 per 1000 males with an overall prevalence of 0.8%.
Morbidity typically results from failure to make the diagnosis of hypothyroidism and failure to institute l-thyroxine replacement therapy in adequate doses or failure on the part of the patient to take the replacement medication.
The symptoms of Hashimoto's thyroiditis are similar to those of hypothyroidism in general, which are often subtle. They are not specific (which means they can mimic the symptoms of many other conditions) and are often attributed to aging. Patients with mild hypothyroidism may have no signs or symptoms. The symptoms generally become more obvious as the condition worsens and the majority of these complaints are related to a metabolic slowing of the body.
As hypothyroidism becomes more severe, there may be puffiness around the eyes, a slowing of the heart rate, a drop in body temperature, and heart failure. In its most profound form, severe hypothyroidism may lead to a life-threatening coma (myxedema coma ). In a severely hypothyroid individual, a myxedema coma tends to be triggered by severe illness, surgery, stress, or traumatic injury. This condition requires hospitalization and immediate treatment.
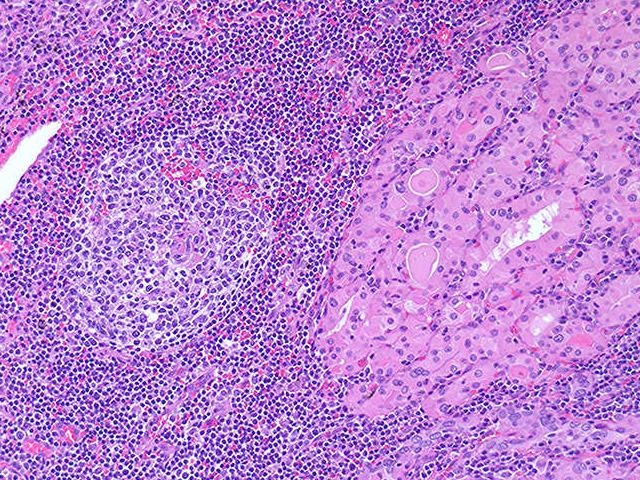 Image Description: A dense infiltrate of plasma cells and lymphocytes with germinal center formation is seen in this thyroid. Cells of the individual colloid follicles often display abundant pink granular cytoplasm, which is referred to as oncocytic change, in this setting. These cells are referred to as Hurthle cells or oncocytes - these are metaplastic.
Image Description: A dense infiltrate of plasma cells and lymphocytes with germinal center formation is seen in this thyroid. Cells of the individual colloid follicles often display abundant pink granular cytoplasm, which is referred to as oncocytic change, in this setting. These cells are referred to as Hurthle cells or oncocytes - these are metaplastic.
RISK FACTORS AND CAUSES
Hashimoto's thyroiditis is a condition caused by inflammation of the thyroid gland. It is an autoimmune disease, which means that the body inappropriately attacks the thyroid gland––as if it was foreign tissue. The underlying cause of the autoimmune process still is unknown. Hashimoto's thyroiditis tends to occur in families, and is associated with a clustering of other autoimmune conditions such as Type 1 diabetes, and celiac disease. Hashimoto's thyroiditis is 5–10 times more common in women than in men and most often starts in adulthood. Blood drawn from patients with Hashimoto's throiditis reveals an increased number of antibodies to the enzyme, thyroid peroxidase an enzyme (protein) found within the thyroid gland. As result of the antibodies' interaction with the enzyme, inflammation develops in the thyroid gland, the thyroid gland is destroyed, and the patient ultimately is rendered hypothyroid (too little thyroid hormone).

PATHOGENESIS
Hashimoto thyroiditis is characterized by the destruction of thyroid cells by various cell- and antibody-mediated immune processes. The initiating process is not well understood. The thyroid gland is typically goitrous but may be atrophic or normal in size. Antibodies binding to and blocking the thyroid-stimulating hormone (TSH) receptor have also been described and may contribute to further impairment in thyroid function. The result is inadequate thyroid hormone production and secretion, although, initially, both preformed thyroxine (T4) and triiodothyronine (T3) may "leak" into the circulation from damaged cells.
Patients with Hashimoto thyroiditis have antibodies to various thyroid antigens, the most frequently detected of which include antithyroid peroxidase (anti-TPO), antithyroglobulin (anti-Tg), and, to a lesser extent, TSH receptor-blocking antibodies. Nevertheless, a small percentage of patients with Hashimoto thyroiditis (approximately 10-15%) may be antibody negative.
Other antithyroid antibodies found in AITD (including Hashimoto thyroiditis) include thyroid-stimulating antibody and cytotoxic antibody.
Other variants of AITD include the following conditions:
Atrophic thyroiditis;
Juvenile thyroiditis ;
Postpartum thyroiditis;
Silent thyroiditis;
Focal thyroiditis.

DIAGNOSIS
In diagnosing Hashimoto's thyroiditis, a physician should assess symptoms and complaints commonly seen in hypothyroidism, examine the neck, and take a detailed history of family members. Blood tests are extremely useful in diagnosing Hashimoto's thyroiditis. The blood tests look at the thyroid function in general. (With hypothyroidism, a high thyroid stimulating hormone and low thyroid hormone would be expected.)
When hypothyroidism is present, the blood levels of thyroid hormones can be measured directly and are usually decreased. However, in early hypothyroidism, the level of thyroid hormones (T3 and T4) may be normal. Therefore, the main tool for the detection of hyperthyroidism is the measurement of the TSH, the thyroid stimulating hormone. As mentioned earlier, TSH is secreted by the pituitary gland. If a decrease of thyroid hormone occurs, the pituitary gland reacts by producing more TSH and the blood TSH level increases in an attempt to encourage thyroid hormone production. This increase in TSH can actually precede the fall in thyroid hormones by months or years (see the section on Subclinical Hypothyroidism below). Thus, the measurement of TSH should be elevated in cases of hypothyroidism. However, there is one exception. If the decrease in thyroid hormone is actually due to a defect of the pituitary or hypothalamus, then the levels of TSH are abnormally low. As noted above, this kind of thyroid disease is known as "secondary" or "tertiary" hypothyroidism. A special test, known as the TRH test, can help distinguish if the disease is caused by a defect in the pituitary or the hypothalamus. This test requires an injection of the TRH hormone and is performed by an endocrinologist (hormone specialist).
The blood work mentioned above confirms the diagnosis of hypothyroidism, but does not point to an underlying cause. A combination of the patient's clinical history, antibody screening (as mentioned above), and a thyroid scan can help diagnose the precise underlying thyroid problem more clearly. If a pituitary or hypothalamic cause is suspected, an MRI of the brain and other studies may be warranted. These investigations should be made on a case by case basis.
The blood tests also usually include an analysis of antibodies (anti–thyroid peroxidase antibodies) to aid in the diagnosis.
If the gland is large– or there are symptoms of esophageal compressive, an ultrasound may be performed to see if the gland is compressing either the esophagus or the trachea (the food and breathing pipes).

THERAPY
There is no cure for Hashimoto's thyroiditis. There is no way to know how long the autoimmune process and inflammation will continue. In the vast majority of patients, hypothyroidism results from the inflammatory process.
Thyroid hormone medication can replace the hormones the thyroid made before the inflammation started. There are two major thyroid hormones made by a healthy gland (T3 and T4). Replacing one or both of these hormones can alleviate the symptoms caused by the absolute or relative lack of hormones as a consequence of Hashimoto's thyroiditis. Without medication, there is very little chance the thyroid would be able to maintain hormone levels within the normal range, and symptoms and signs of hypothyroidism would occur or worsen.
- Normal thyroid (Left)
- (Right) Struma lymphomatosa in Hashimoto thyroiditis, gross. Note: diffuse, pale yellow infiltrate affecting the entire thyroid. The yellow infiltrate is caused by an influx of lymphocytes, which may form follicles.