Vaginismus , sometimes called vaginism, is a persistent and an involuntary spasm of the perineal muscles, which close the vagina. It's the condition that affects a woman's ability to engage in any form of vaginal penetration (sexual penetration, insertion of menstrual cups and tampons and gynecological examinations. ( Successful management of vaginismus: An eclectic approach, 2011 )


Epidemiology:
Vaginismus is an uncommon condition, which affects 1-7% of women all around the world.
A study in women in Sweden and Morocco revealed a prevalence of 6%. 18-20% of women in British and Australian studies manifested dyspareunia, while the rate among elderly British women was as low as 2%.
A 1990 study of women presenting to sex therapy clinics found reported vaginismus rates of between 12% and 17%, while a random sampling and structured interview survey conducted in 1994 by National Health and Sexual Life Survey documented 10%-15% of women reported that in the past six months they had experienced pain during intercourse.
The most recent study-based estimates of vaginismus incidence range from 5% to 47% of people presenting for sex therapy or complaining of sexual problems, with significant differences across cultures .
Symptoms:
The main symptoms are:
Difficult, painful, or impossible, vaginal penetration during sex
Vaginal pain during sexual intercourse or a pelvic exam
This patology ( whose severity varies from woman to woman ) is caused by a reflex of the pubococcygeous muscle( "PC muscle" ),that makes the muscles in the vagina tense suddenly, which makes any kind of vaginal penetration painful or impossible.
The vaginismic reflex can be compared to the response of the eye shutting when an object comes towards it.
A woman suffering from vaginismus isn't able to consciously control the spasm. Spasm may be due to muscles around the pelvis being tight from the frequent tension. This also limits blood flow through the whole vaginal area. This makes the mucous membranes sensitive and prone to tearing. This is painful to different degrees and means that some women experience pain in their daily lives and sometimes they are unable to ride a bicycle or even wear jeans.
Women affected by this patology often become anxious about sexual intercourse; However the most of those women are turned on sex and ,despite of their conditions, they can have orgasms when the clitoris is stimulated.
Diagnosys:
A pelvic exam can confirm the diagnosis of vaginismus. A medical history and complete physical exam are important to look for other causes of pain with sexual intercourse ( dyspareunia )
Patogenesis:
An important role in this mechanism of pelvic muscolar contraction is covered by the release of Acetylcholine on neuromuscolar junctions:


Acetylcholine is a neurotransmitter involved in the stimulation of muscle tissue, by binding to the nicotinic acetylcholine receptor (AChR) ,a ligand-gate channel of eucaryotic cells.
AchRs, located at the skeletal neuromuscular junction, form heteropentamers comprised of two α, one β, one γ, and one δ subunits. When a single ACh ligand binds to one of the α subunits of the ACh receptor it induces a conformational change at the interface with the second AChR α subunit. This conformational change results in the increased affinity of the second α subunit for a second ACh ligand. AChRs therefore exhibit a sigmoidal dissociation curve due to this cooperative binding .The presence of the inactive, intermediate receptor structure with a single-bound ligand keeps ACh in the synapse that might otherwise be lost by cholinesterase hydrolysis or diffusion.
The persistence of these ACh ligands in the synapse can cause a prolonged post-synaptic response on the neuromuscular junction, which can be even increased by Adrenalyne and can increase muscolar spasms.
The mechanism of muscolar contraction is the following:

1. Upon the arrival of an action potential at the presynaptic neuron terminal, voltage-dependent calcium channels open and Calcium ions flow from the extracellular fluid into the presynaptic neuron's cytosol.
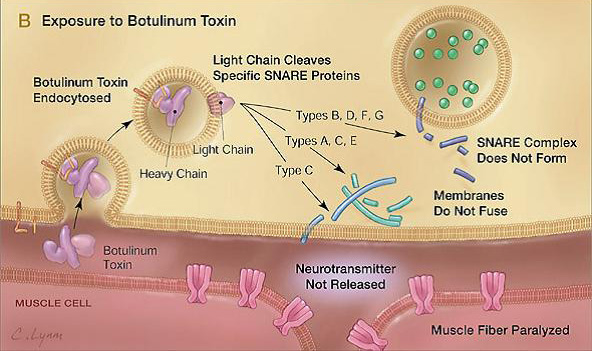
2. This influx of Calcium causes neurotransmitter-containing vesicles to dock and fuse to the presynaptic neuron's cell membrane through SNARE proteins.
3. Fusion of the vesicular membrane with the presynaptic cell membrane results in the emptying of the vesicle's contents (acetylcholine) into the synaptic cleft, a process known as exocytosis.
4. Acetylcholine diffuses into the synaptic cleft and can bind to the nicotinic acetylcholine receptors on the motor end plate.
5. These receptors are ligand-gated ion channels, and when they bind acetylcholine, they open, allowing sodium ions to flow in and potassium ions to flow out of the muscle cell.
6. Because of the differences in electrochemical gradients across the plasma membrane, more sodium moves in than potassium out, producing a local depolarization of the motor end plate known as an end-plate potential (EPP).
7. This depolarization spreads across the surface of the muscle fiber and continues the excitation-contraction coupling to contract the muscle.
8. The action of acetylcholine is terminated when ACh diffuses away from the synapse or the enzyme acetylcholinesterase degrades part of ACh (producing choline and an acetate group).
9. The choline produced by the action of acetylcholinesterase is recycled — it is transported, through reuptake, back into the presynaptic terminal where it is used to synthesize new acetylcholine molecules.
Patient Risk Factors:
Vaginismus has several possible causes, including past sexual trauma or abuse,psychological factors and history of discomfort with sexual intercourse.
A few of the main factors that may contribute to primary vaginismus include:
- a condition called vulvar vestibulitis syndrome, more or less synonymous with focal vaginitis, a so-called sub-clinical inflammation, in which no pain is perceived until some form of penetration is attempted.
- urinary tract infections
- vaginal yeast infections
- sexual abuse, rape, other sexual assault, or attempted sexual abuse or assault
- knowledge of (or witnessing) sexual or physical abuse of others, without being personally abused
- domestic violence or similar conflict in the early home environment
- fear of pain associated with penetration, particularly the popular misconception of "breaking" the hymen upon the first attempt at penetration, or the idea that vaginal penetration will inevitably hurt the first time it occurs
- personality traits such as pain-catastrophizing cognitions[clarification needed] and harm-avoidance behaviour
- any physically invasive trauma (not necessarily involving or even near the genitals)
- generalized anxiety
- stress
- negative emotional reaction towards sexual stimulation, e.g. disgust both at a deliberate level and also at a more implicit level
- strict conservative moral standards with low liberal moral standards a general difficulty at doing 'wrong' or behaving in ways perceived as transgressive, which also can elicit negative emotions ( Vaginism, 2007 )
Complications:
There are many levels of severity. The understanding of this by clinicians and patients alike is important so that the proper treatment can be instituted.
In 1978, Lamont described a classification of vaginismus to describe the severity of the vaginismus. His findings were based both on the history of the patient and observations during an attempted GYN examination. All patients gave a history of painful intercourse and all vaginismus patients were noted to have generalized tightness of the pelvic floor. In 2010, Dr. Pacik expanded the Lamont classification by introducing a Level 5 vaginismus (see references below).
Lamont described the following breakdown:
- First degree vaginismus as spasm of the pelvic floor that could be relieved with reassurance and the patient could relax for her examination.
- Second degree vaginismus, generalized spasm of the pelvic floor as a steady state despite reassurance, and the patient was unable to relax for the exam.
- Third degree vaginismus, the pelvic floor spasm was sufficiently severe that the patient would elevate the buttocks in an attempt to avoid being examined.
- Fourth degree vaginismus, the most severe form of vaginismus described by Lamont, the patient would totally retreat by elevating the buttocks, retreating, and tightly closing the thighs to prevent any examination.
- Pacik described 5th degree vaginismus as a visceral reaction manifested by increased adrenalin output and resulting in any of the following: Increased heart rate, palpitations, hyperventilation, trembling, shaking, nausea or vomiting, crying uncontrollably, a feeling of light headedness and fainting, a desire to jump off the table, run away or even attack the doctor. ( Lamont Classification, 2013 )
Therapy:
The treatment required can depend on the reason that the woman has developed the condition:it involves a combination of education, counseling, and exercises such as pelvic floor muscle contraction and relaxation (Kegel exercises).
Vaginal dilation exercises are recommended using plastic dilators. These should be done under the direction of a sex therapist or other health care provider. Therapy should involve the partner. It can gradually include more intimate contact, ultimately leading to intercourse.
Recent results have suggested the use of botulinum toxin for the treatment of vaginismus.Vaginal Botox injections for the treatment of vaginismus has received increasing attention since the technique was first described in a 1997 case report.

Botox is well known to help reduce or eliminate muscle spasm and for this reason is used for the treatment of vaginismus, especially the more severe cases when patients say that intercourse is like "hitting a wall". In cases of vaginismus where more traditional treatments have not been successful, a paralytic agent such as Botox may be used. Botox offers an option that allows women who deeply fear penetration to the point where probes are "too scary" to move ahead despite this fear. The use of Botox relaxes the muscle spasm for about four months. Optionally, if the procedure is carried out under sedation or general anesthesia, the patient may awaken having already achieved what is usually the hardest first step: the insertion of a probe. The anesthesia works in concert with the Botox injection(s) to ensure that her first experience with the probe is not painful. ( Vaginismus: review of current concepts and treatment using botox injections, bupivacaine injections, and progressive dilation with the patient under anesthesia, 2011 )