Is a coffee break a good idea to relive migrain symptoms? Caffeine seems to both causes and relieve migraine symptoms, how is it possible? That is the so-called caffeine paradox.
Introduction
Caffeine can be found in over 100 species of plants. Probably plants produce caffeine as a protective agent against insects, that happens thanks to the effect of the molecule wich suppress insect appetite and inhibits their ability to eat acting on their nervous system. Plant-eating animals, on the orher side, have to protect themself from the activity of neurotoxical alchaloids: one way is to detect and avoid the dangerous substance (eg. the bitter taste is a clue of the presence of a toxic substance), another strategy consists in adapting and adjusting the nervous system in order to have a normal functionality despite the presence of the neurotoxic substance. The adaptation, however, comes at price of the so called migraine-like caffeine withdrawal. Caffeine and Migraine - 1996-2010

Molecular Role
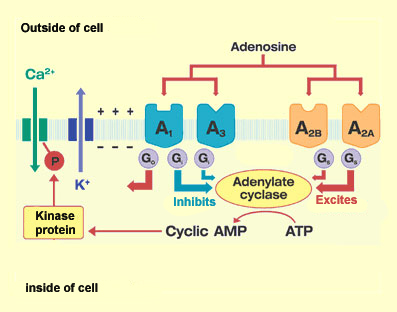
Caffeine is a neurotoxic alkaloid able to occupy and block adenosine receptors (ARs) thanks to its shape, very similar to adenosine structure. Caffeine, therefore, prevents adenosine to bond to its receptor blocking its action. The adenosine A1 and A2A receptors have high affinity for adenosine and are those responsible for tonic actions of endogenous adenosine. Adenosine is present in all cells and AR can be foud in brain cells, so , any imbalance in this widespread system is expected to lead to neurological disfunction. While acting as an AR antagonist, caffeine lower the levels of the endogenous and tonically activity of adenosine. Adenosine act as tranquillizer decreasing the release of excitatory neurotrasmitter regulating synapses through tuning and fine-tuning. Tuning synapses occurs when adenosine regulates the release of neurotransmitters, by interfering with Ca2+ or other mechanisms directly related to neurotransmitter release. In the case of fine-tuning adenosine is interfering with receptors for other neuromodulators. Peripherally adenosine causes pain and vasodilation (expecially in the vessels of head and neck). Caffeine, interfering with Adenosine activity by blocking its acces to AR, has opposite effects: it is a vasoconstrictor and enhance the release of excitatory neurotrasmitter, that's why caffeine is stimulating. Besides AR antagonism, xanthines, including caffeine, have other biological actions, such as inhibition of phosphodiesterases (PDEs), promotion of calcium release from intracellular stores, interfering with GABA-A, ACh, Serotonin, Dopamine, Norepinephrine receptors. However, in the case of caffeine, the effects seen at very low doses, achieved during normal human consumption, are mostly due to AR antagonism. Because of its safety, its ability to antagonize ARs and to readily cross the blood brain barrier, caffeine has therapeutic potential in central nervous system dysfunctions. Adverse effects of caffeine may include anxiety, hypertension, drug interactions, and withdrawal symptoms. Therapeutic and adverse effects are strictly dependent on wether caffeine is administered chronically or acutely. A chronic assumption in everyday life causes a mechanism of adaptation to restore the levels of the adenosine's activity that leads to:
- increase in numer of ARs; (mainly A1)
- increase in the affinity of those receptors;
- decrease the rate of the reuptake of adenosine from synapses (increasing the number of membrane transporters).
This adaptation is responsible of a stronger response to adenosine to compensate the action of caffeine that blocks a percentage of AR. Caffeine and Adenosine - 2013
Migrain and the caffeine paradox
Migraine is a chronic neurological disorder characterized by recurrent moderate to severe headaches often in association with a number of authonomic nervous system symptoms. The caffeine's paradox is that it seems to both cause and relieve headaches. There are several theories that explain the benefical effect of caffeine in migrainers. Wikipedia/Migraine - 2012
The vascular theory
In most cases migrain headaches are pounding headaches, with pain spiking in time with the pulse. According to the vascular theory, vascular constriction in the brain causes ischemia, which causes aura symptoms, followed by vascular dilation that causes the head pain. The brain itself is insensitive to pain, so the vascular theory postulates that migraine pain originates when dilated blood vessels in the meninges press against or otherwise physically or chemically irritate sensory nerves. The vascular theory has problems:
- blood vessels routinely constrict and dilate without causing pain;
- vascular constriction that happens during migraine episodes doesn't choke off cerebral blood flow enough to cause aura symptoms;
- an experiments in which blood pressure in the brain was artificially increased failed to produce migraine-like symptoms;
- the central problem with the vascular theory, however, is that it assumes vascular changes cause migraine symptoms, when there are other logical possibilities: the headache could cause the vascular dilation, or a third factor could cause both the vascular dilation and the headache.
Adenosine, by inhibiting the release of norepinephrine from neurons (the neurotrasmitter wich causes vasocostriction), causes vasodilation (see III in the image). Caffeine, by blocking adenosine, prevents adenosine from inhibiting norepinephrine release, so caffeine increases the amount of norepinephrine released by neurons, and thereby causes vasoconstriction (see II in the image). Adenosine is the likely culprit behind both the vasodilation and pain. Migraine is a derangement of normal neurochemical mechanisms, including those that control blood vessel diameter. During a migraine episode, the blood concentration of adenosine in the head and neck is elevated quite a bit above normal. Adenosine causes pain and is a potent vasodilator, so it's not surprising that excessive adenosine in the head is associated with the head pain and vascular dilation that typically accompany migraine episodes. Nor is it surprising that caffeine, which blocks adenosine, remedies headache. Caffeine and Migraine - 1996-2010

Adjuvant Theory
Another theory is that caffeine in combination headache medicines works by enhancing the effects of the medicines it's combined with. One proposed mechanism for the adjuvant effect of caffeine is that caffeine expedites delivery of the other medicines by speeding up absorption of the medicines through the gut wall into the bloodstream, or by increasing heart rate, thereby speeding the hero medicines on their way.
The adjuvant theory doesn't explain why caffeine all by itself often effectively aborts headache, and has an analgesic effect on headache independent of other medicines. Moreover, because oftentimes caffeine all by itself aborts headache, the so-called adjuvant or synergistic effect of caffeine would be difficult to demonstrate. If a caffeine-containing combination headache medicine aborts a headache, it would be hard to determine how much of the credit goes to an adjuvant effect of caffeine rather than to the intrinsic ability of caffeine to abort headache. But caffeine does slow the rate at which aspirin and acetaminophen (paracetamol, Tylenol) are metabolized, so could make aspirin and acetaminophen more effective by keeping them in the body longer and at a higher concentration.

curves for acetylsalicylic acid (ASA) alone (squares) and combined with caffeine (CAF, triangles), on the inhibition of mechanical hyperalgesia (%
MPE), 3 h after CA-induced inflammation. Each point represents mean values of at least eight rats and vertical bars indicate
SEM. ∗ indicates statistically significant differences (p < 0.05; Student’s t test) between treatments. It is evident that the same dose of
ASA combined with
CAF has greater effects that
ASA alone.
European Journal of Pain - 2008
How caffeine can cause migraine
Chronical caffeine assumption causes an adaptation mechanism (see Molecular Role) that makes the nervous system dependent on caffeine. Due to the adaptation caused by caffeine the migrainer is more sensitive to adenosine activity on receptors and insensitive to excitatory neutransmitter (thanks to the inhibitory activity of adenosine). Caffeine, therefore, alter the nervous system right way to make a person migrainer. When the individual ceases the intake of caffeine the remaining caffeine is catabolized by the liver. Without the regular dose of caffeine, adenosine has a free access to its receptors previously blocked, that cause an over-response, due to an excessive number of AR and an excessive sensivity, that lead to:
- migrain-like caffeine withdrawal headache;
- a decrease of excitatory trasmitter activity (eg. a shortage of serotonin receptor activation prevent serotonin to block pain, a shortage of ACh in the retina causes visual disturbance associated with migrain, a shortage of dopamine causes an alteration in the behaviour, a shortage of norepinephrine cause a disfunction in the sympathetic nervous system activity)
- vasodilation of the vessels in the neck and in the head (see Vascular Theory).
Predisposition to migraine
- Family History: Genetic factors play a large role in those suffering from migraine headaches. Studies have shown up to 90 percent of people with migraine headaches have a family history of them and studies say that those individuals that come from a family history of migraine headaches will most likely be at risk of suffering from chronic migraine headaches as well.
- Age: During childhood, migraine headaches are less frequent but not nonexistent. Research has shown that most individuals will experience their first migraine headaches during adolescence, and by age 40, most people who will suffer from migraine headaches will have had their first attack.
- Gender: It is a commonly known fact that more people who suffer from migraine headaches tend to be female. Hormonal changes seem to play a very large role in the case of migraines. During childhood or adolescents, the frequencies of migraine headaches between sexes were not that different but a drastic increase in migraine headaches in females become apparent as they neared puberty. The reason behind this statistic seems to reside in the case of estrogen, its levels, and its effects on migraine headaches. This is also why women often complain more of migraines around the time of their monthly cycle.
- Medical Issues: Individuals who are have medical issues such as depression, anxiety; stroke, epilepsy and high blood pressure are more susceptible to migraine headaches than people who have not suffered with any of the listed medical concerns.
Is Predisposition To Migraines Real? - 2012
Conclusion
According on the previous views, the caffeine paradox is explained assuming that caffeine causes headaches by provoking neurochemical dependency due to adaptation events, the nervous system, therefore, became susceptible to caffeine withdrawal headaches, caffeine relieve migrain reversing the effects of abstinence, causing vasoconstriction (as an antagonist of adenosine vasodilation activity) and by adjuvating the effects of analgesic drugs.