DESCRIPTION
Salbutamol is a β2- synthetic agonist principle, with direct action, ingredient of many drugs, useful for several therapeutic treatment, mainly for the relief of bronchospasm in conditions such as asthma and chronic obstructive pulmonary disease. It is marketed as Ventolin among other brand names.

CLASSIFICATION
It is a sympatic mimetic principle, β2 adrenergic selective.
Molecular formula C 13 H 21 NO 3
Synonymous:
- albuterol
- alpha1-[[(1,1-Dimethylethyl)-amino]methyl]-4-hydroxy-1,3-benzenedimethanol
- alpha1-[(tert-butylamino)methyl]-4-hydroxy-m-xylene-alpha,alpha'-diol
- 2-(tert-butylamino)-1-(4-hydroxy-3-hydroxymethylphenyl)ethanol
- 4-hydroxy-3-hydroxymethyl-alpha-[(tert-butylamino)methyl]benzyl alcohol
About the chemical structure of the symphatetic-mimetics, the fenil-ethylamine can be considered the compound they come from. It is composed by a benzene ring with an ethylaminic lateral chain.
!
http://www.vilaglex.hu/Kemia/Kepek/Pea.gif
!
Starting from it, substitutions can be made:
- On the benzene ring: the salbutamol shows substitutions at level of positions 3, an hydroxide-methyle, and 4, an hydrophile.
These substitutions allow the adrenergic activity: in these locations all the cathecholamines show two hydrophilic groups.
- On the alpha carbon: they prevent the oxidation of the monoaminoxidase MAO, prolonging the drug action.
This one is not present on the cathecholamines, which need a temporary activity, while it is important on the medecines.
- On the amino group: more the size of the alchilic substitute grows, more the β activity grows, too.
Indeed, the salbutamol is provided with β selectivity, particularly β 2, as it manifests substitution of 3 methyl groups: hysopropylic substitution. It’s the substitution which awards the most β selectivity, in particular β 2.
INDICATIONS
The salbutamol, acting on the β2 receptors, is able to promote the relaxation of the unstriated musculature in breathing apparatus, in uterus, and in the vessels of some vascular districts.
Other functions are to promote che the grasp of potassium at the level of the skeletal muscle and to increase the glycogenolysis at hepatic level.
Thanks to these activities the salbutamol is mainly used as bronchus-expandable, tocolytics and hypo-kaliemizzante.
PHARMACOKINETICS
Distribution:
Oral way: salbutamol is easily absorbed into the gastric-intestinal section. The pharmacological effect appears 30 minutes after the oral ingestion, join the top within 2-3 hours and continues for 6 hours about (Martindale, 1996).
After administration of pharmaceutical control-releases forms, the pharmacological action persist for about 12 hours.
Plasmatic peak: 3 hours.
Administration by inhaling: the pharmacological effect appears in 5-15 minutes, join the top in 60-90 minutes and continues for 4-6 hours. Such administration allows to soften the metabolic collateral effect, and those on the cardiovascular system, which can arise after oral and parenteral administration (Bateman et al., 1978).
Salbutamol doesn’t permeate the hematoencephalic barrier.
Metabolism:
It is bio-transformed into the liver and into the intestine, where it’s metabolized through combination with sulfate groups, starting the inactive form of ester 4’-O-sulfate, due to the phenol- sulphur-transferase (PST).
Into the lung it doesn’t take place bio-transformation reactions, so, after inhalatory administration, the destination of the drug depends on its formulation which defines the quantity of salbutamol that is accidentally swallowed.
Excretion:
It is excreted through the urine till the 78% in 24 hours after a single oral dose and till the 89% after a inhalated dose; it is excreted for the 50% in combined form and for the 50% unmodified.
http://www.pharmamedix.com/principiovoce.php?pa=Salbutamolo&vo=Farmacocinetica
http://toxnet.nlm.nih.gov.offcampus.dam.unito.it/cgi-bin/sis/search
Posology:
Usually, for the asthma therapy, the anedrergic agonists are better emitted through inhaling, because it involves the biggest local effect along with the smallest systemic toxicity. The deposition of aerosol depends on the dimensions of the particles, on the profile of the breath and on the geometry of the air ducts. Even with optimal particles of 2-5 micrometers the 80-90% of the aerosol dose lays down into the mouth and into the pharynx. Particles of 1-2 micrometers stay hanging and can be breathed out. The bronchial deposit can be increased slowly inhaling until the total lung capacity and keeping the breath for more than 5 seconds at the end of the inhalation.
The salbutamol is also tablet available, but the oral administration doesn’t bring any advantage for the bronchus-expandable effects.
The salbutamol is also available for intramuscular and intravenous injection, and this way is recommended in event of serious asthma, when the aerosol therapy is not available. This way brings more frequent occurrences of accumulation, with following several effects.
http://www.pharmamedix.com/principiovoce.php?pa=Salbutamolo&vo=Posologia
MOLECULAR MECHANISM
The salbutamol is a sympaticomimetic drug acting in direct way, that is to say it directly interacts with the adrenergic receptors in order to activate them.
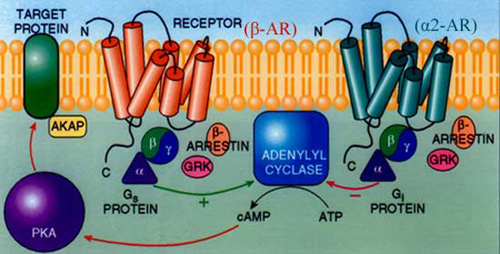
Receptors:
Its effects are mediated by the membrane adrenergic receptors, typical receptors matched with G protein (GPCRs). They show the aminic extra-cellular terminal, 7 trans-membrane domains and the carbossylic intra-cellular terminal. They are coupled through G proteins with several realizing proteins, of whom they govern the activity. G proteins are heterodimers composed by three sub-units, α, β e γ, of which the α sub-unit distinguishes the action of the protein: Gs α works stimulating the adenylate cyclase, Gi α works as inhibitor of this enzyme, and Gq α is a stimulator of C fosfo-lipase.
Intracellular molecular pathways:
The link of an antagonist on these receptors involves an allosteric modification, which promotes the separation of GDP from G protein. The separation keeps it in inactive structure, from a syte of specific connection on α sub-unit. So it promotes the joint of a GTP molecule, which on the contrary starts its functions.
The activation involves the separation of α sub-unit, activated by the link with GTP, by the β – γ complex, and the possibility of activating the effector enzyme during the moving of the intra-cellular signal.
α sub-unit will face an inactivation when its GTP-asica intrinsic activity will lead to hydrolysis from GTP to GDP, carrying its new association with β – γ complex.
Selectivity:
The adrenergyc receptors are pharmacologically defined in αe β. The salbutamol is selective for the β receptors, but the selectivity towards the several sub-types is not very emphasized. Even if it is selective for the sub-type β2, it also presents some level of affinity for β1, realizing its effects on several apparatus, very affected by the concentration it’s able to reach, and by the relative expression of the different sub-types of receptors inside the target tissues.
Also the way of administration which is adopted can influence the effects, because it can lead the drug to locate mainly at the level of specific tissues.
β-receptor's effect:
The β-adrenergic activated receptors, whatever is the sub-type of receptor, act through a Gs α protein, stimulating the adenylate-cyclase, anchorated at the membrane, to produce c-AMP, starting from the ATP.
The increase of c-AMP allostericly activates the kinase A protein (PKA), a Serin Threonin kinase, which catalyses the phosphorylation of other proteins, manifesting sites with Serin or Threonin susceptible.
http://toxnet.nlm.nih.gov.offcampus.dam.unito.it/cgi-bin/sis/search/f?./temp/~4NbiT6:1indicazioni
PHARMACOGENOMICS
Bronchus-expandable effects:
It is due to its effects on the unstriated musculature, in specific on the bronchial one, which myositis mainly express β2 receptors: it is the tissue which mainly express these types of receptors, in consequence this one is the main effect of salbutamol.
The PKA may phosphorylate the kinase of the light chain of myosin (MLCK): in its phosphorylate inactive form it is not able anymore to phosphorylate the light chain of myosin, not allowing the connection with actin and the following muscular contraction. With this working the myositis go forward a relaxation producing the bronchus-expansion.

The agonist adrenergic β2 selective medecines, like salbutamol, are the symphatetic-mimetic medecines presently most employed in the therapy for chronic obstructive bronchus-pneumopathies (BPCO) like asthma.
They express this result in an effective way, after inhalatory administration or by orally, and thanks to their long duration action.
More, the salbutamol runs to inhibition of releasing of bronchus-constrictors mediators by the side of mascocytes, leading to an increase of cAMP into the luco-cytoplasm.
Tocolytic effect:
It induce a relaxation of the unstriated uterine musculature, with the same work of the bronchial one.
Hypo-kaliemizzante effect:
The salbutamol increase the catching of potassium by the skeletal muscle.
This event is also responsible for the collateral effect of salbutamol to cause skeletal muscles trembles.
This actions depends on specific ionic channels, modulated by cyclic neuclotides called HCN. These channels are weakly selective for potassium, and are modulated in the direction of a greater probability of opening from cAMP, with the possibility of having bigger coming flowings of potassium.
This kind of channels is well declared at level of the skeletal muscle cells.
http://www.pharmamedix.com/principiovoce.php?pa=Salbutamolo&vo=Indicazioni
http://toxnet.nlm.nih.gov.offcampus.dam.unito.it/cgi-bin/sis/search/f?./temp/~sclfou:1
http://www.pharmamedix.com/principiovoce.php?pa=Salbutamolo&vo=Farmacologia
SIDE EFFECTS
Interactions:
The problems related with the interaction with other substances come from the fact that the action of salbutamol could be empowered or cancelled.
http://www.pharmamedix.com/principiovoce.php?pa=Salbutamolo&vo=Interazioni
Special warning and controindication:
http://www.pharmamedix.com/principiovoce.php?pa=Salbutamolo&vo=Controindicazioni
http://toxnet.nlm.nih.gov.offcampus.dam.unito.it/cgi-bin/sis/search
http://www.pharmamedix.com/principiovoce.php?pa=Salbutamolo&vo=Avvertenze
http://toxnet.nlm.nih.gov.offcampus.dam.unito.it/cgi-bin/sis/search
Doping:
Due to the effects they exert, the β-antagonist drugs are in the category of the doping substances. Particularly, the bronchus-expandable and ino/coronotropy effects, positives at cardiac level, give decisive results in the physical performance. More than this working, they also induce vessel dilation at the level of muscular skeletal tissue, provisioning a better performance.
Side effect:
Atrial Fibrillation
TOXICITY
Damaging effects may rise, as collateral effect of the normal therapeutic use, only if chronic, with accumulation events, but the more frequent toxicity examples are related with overdosage events, which allows to rise high concentrations of salbutamol, so losing the β 2 selectivity.
Overdosage:
In the event of overdosage, irritability, hypersweating, tachycardia, headache, tremors, vomit, hypotension, arrhythmia, hypopotassemia and hyperglycaemia may arrive.
The therapy considers: gastric lavage if the administration was by oral way; administration of β-antagonist (with extreme care if asthmatic or bradycardic patients); infusion of liquid by intravenous injection; administration of diazepam if convulsions arrive (till 10 mg slowly injected to the adult, 0,1-0,3 mg/Kg to the child). Furthermore, monitor the pressure, the cardiac function and the electrolytic concentration.
DL50: After oral administration: more of 2000 mg/Kg in the rat and in the male and female mouse.
Toxical effects at cardiovascular level:
Tachycardia (in patients with normal cardiac frequency), bradycardia (in patients with preexisting sinusal tachycardia), arhythmia, hypertension or peripheral vessel dilatation with resulting reduction of the arterial pressure, myocardial ischemia.
Even if the most of the warnings of myocardial ischemia – associated with salbutamol – have been observed in patients processed with the drug in case of premature childbirth, the risk of ischemia could interest also the patients who take the salbutamol for breathing diseases.
General effects:
The direct effects on the heart are mostly caused by β-1 receptors, even if also β-2 can contribute in a minor way. In general the activation of these receptors brings an increase of the entry of calcium into the cells, which has consequences either on the electrical properties or on the mechanical ones. The pacemaker activity, as well as the conduction system, is increased and the resistant period is reduced (positive chronotrope effect). The intrinsic contractility is increased (inotrope positive effect) and either the release is hastened (lusitropic positive effect).
Furthermore, it can be responsible for some soft hypotension effects, as consequence of its ability to relax the unstriated vascular musculature, especially into the district which sprinkle the skeletal muscle:
Inotrope and lusitropic positive effects:
- The PKA phosphorilates the calcium L voltage-depending channels at the level of the plasma membrane, increasing its probability of opening, and so increasing the entity of the entering calcium flowing, during the depolarization.
- The activity of these channels is also positively modulated by the direct link of cAMP, which fastens with the calcium channels responsible for the pacemaker current, which brings the potential at threshold for the onset of an action potential.
- The PKA also phosphorilates the ryanodine calcium channels, present on the sarcoplasmatic reticulum, increasing the opening opportunity.
- Furthermore, it phosphorilates the phospholamban, inactivating its function of inhibitor of calcium ATPasis of the sarco-endoplasmatic reticulum SERCA.
- It phosphorilates the troponin, supporting the dissociation of calcium from it.
The capacities to quickly increase and decrease the intra-cell calcium concentrations, and also to arrive to high levels of them, are responsible for the inotrope and lusitrope positive effects, which appears at the level of the working myocytes.


Chronotrope effect:
- The PKA also phosphorilates the potassium Kir channels, responsibles for the hyperpolarisation into the conduction myocytes. The depolarization depends on calcium currents, therefore the workings actings to facility it are the mentioned ones.
The greater ability to quicly depolarize and hyperpolarize the membrane is the base for the cronotrope positive effect.
Effects on the metabolism:
- The β receptors activation into the adipose cells brings to an increase of the lipolysis with following growing release into the circulation of fat acids and glycerol.
- More, they increase the glycogenesis into the liver, with following greater release of glucose into the blood.
Hyperglycemia is observed following IV albuterol administration, with diabetic ketoacidosis occurring in susceptible individuals. Diabetic patients treated with albuterol should, therefore, be under close surveillance and have their insulin dosage increased.
- The activation of β 2 receptors also supports the captation of potassium into the cells, especially into the skeletal muscle cells.
Significant hypokalemia can occur following intravenous or oral administration of albuterol in high doses. The fluctuation in potassium has averaged 10% and 25% with very high doses by inhalation or oral and intravenous doses of albuterol.
At level of the pancreatic islands the β receptors mediate an increase of the insulin release.