CANNABINOIDS IN GLAUCOMA PREVENTION AND TREATMENT
General description of glaucoma and cannabinoids receptors
Glaucoma is a major blinding disease, the second leading cause of loss of sight in the USA. The chief mechanism is excessive pressure inside the eyeball. Treatments focus on reducing this pressure, often through trying to reduce production of the intraocular liquid, aqueous humor, or to increase its drainage.
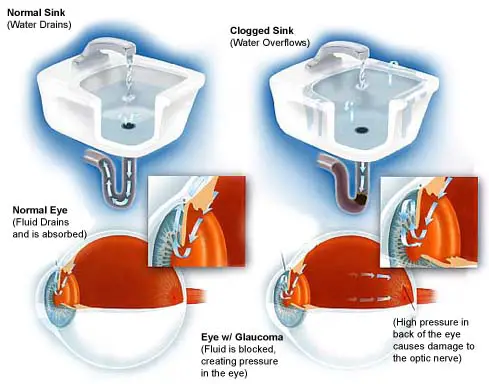
Imagine inflating a basketball to twice its recommended pressure. Not only would it bounce and handle poorly, it would also be in some danger of exploding. In the eye, excess pressure can deform the back of the eyeball where the optic nerve leads deep into the brain. The pressure can cause "cupping", and with it, irreversible optic nerve damage. The crushing effect causes excitotoxicity in the damaged retinal ganglion cells, and further injury results from this oxidation stress.
The function of cannabinoids in lowering this damaging interocular pressure is well known; the treatment of glaucoma with cannabis is one of the most readily identified medical uses of marijuana. Now it is clear that the benefits go far beyond this crucial lowering of intraocular pressure. Activation of the endocannabinoid receptor system also now appears to provide robust neuroprotective effects. Not only does cannabis lower eye pressures, it also serves to help protect the visual nerve cells from damage.
There are two main classes of cannabinoid receptors, known as CB1 and CB2. The CB1 receptors are found mostly in the central nervous system, and these are linked with the psychotropic side effects of cannabis.The CB2 receptors are found mainly in the periphery, notably in the immune system, but are also found sparingly in the brain. In addition, some evidence suggests the existence of a third group of receptors, whose properties are as yet dimly perceived.
Both the CB1 and CB2 receptors have been found in the eye, in several tissues linked to glaucoma; both receptor types are found in the trabecular meshwork, accounting for the greater part of cannabinoid IOP reduction.
CB1 and CB2 receptor signalling affects the cytoskeleton, causing the cells to 'round up' and become less mobile.This in turn may lead to the reduction in IOP by increasing outflow through the meshwork.
IOP is only part of the problem in glaucoma, and the real buzz about the cannabinoid receptors is that they are also found in other cell types linked to glaucoma – the retinal ganglion cells, and the glial cells at the optic nerve head.This means that targeting the cannabinoid receptors has the potential to interfere with all three prongs of the glaucoma trinity – raised IOP, neurodegeneration and excavation of the optic nerve head.
The degeneration of retinal ganglion cells has long been linked with glutamate excitotoxicity, but the underlying cause is still uncertain. One factor is the absorption of light by the abundant mitochondrial proteins in the ganglion cells, converting them into potent free-radical generators.
The free-radical species most incriminated in ganglion cell death is peroxynitrite, formed when nitric oxide reacts with a superoxide radical. In this context, it's interesting that cannabinoids such as delta-9 THC can protect retinal ganglion cells against peroxynitrite toxicity via a mechanism that involves the CB1 receptors.
The reason it works is that peroxynitrite is only formed when there's plenty of nitric oxide around, which in turn is formed via the enzyme nitric oxide synthase – a calcium- dependent enzyme.
Cannabinoids inhibit calcium signalling in rat retinal ganglion cells.This in turn should block nitric oxide formation, and so protect ganglion cells against excitotoxicity.
Research, reported in Investigative Ophthalmology and Visual Science, found CB1 receptors in all the frontal eye anatomy thought important in controlling IOP (intraocular pressure). These include Schlemm’s canal and “ciliary epithelium, trabecular meshwork, and in the blood vessels of the ciliary body.” The authors surmised that evidence of CB1 receptors in the “ciliary pigment epithelium suggests that cannabinoids may have an effect on aqueous humor production.” CB1 presence in the trabecular meshwork and Schlemm’s canal “suggests that cannabinoids may influence conventional outflow.” Evidence of effects on uveoscleral outflow are inferred by CB1 in the ciliary muscle.

CB1 receptors are also present on the other (back) end of the eye, the all important retina and its attachment to the optic nerve with retinal ganglion cells. Here, the neuroprotective effects of activation of cannabinoid receptors may prevent and reduce damage caused by high IOP. Research out of Finland concluded that “at least some cannabinoids may ameliorate optic neuronal damage through suppression of N-methyl-D-aspartate receptor hyperexcitability, stimulation of neural microcirculation, and the suppression of both apoptosis and damaging free radical reactions, among other mechanisms.”
Not all neuroprotective properties of cannabinoids come from their activation of the endocannabinoid system; cannabinoids are powerful antioxidants in their own right.
Classic cannabinoids such as Δ9-THC, HU-211, and CBD have antioxidant properties that are not mediated by the CB1 receptor. As a result, they can prevent neuronal death by scavenging toxic reactive oxygen species produced by overstimulation of receptors for the excitatory neurotransmitter, glutamic acid.
The British researchers also note that regarding the CB2 receptor, “The anti-inflammatory properties of CB2 receptor agonists might also prove to be of therapeutic relevance in different forms of inflammatory eye disease.”
Localization of Cannabinoid CB1 Receptors in the Human Anterior Eye and Retina
Wikipedia the free encyclopedia
Cannabis and glaucoma-The inside story
A short history of cannabis
Cannabis/marijuana is the most frequent illicit drug used today for recreational purposes. Yet it is not widely known that the cannabis plant (Cannabis sativa; Latin for “planted hemp”) is one of the oldest drugs used for medical purposes. Its therapeutic use was first recorded in a classical medicine book by the Chinese emperor Shen Nung in 2737 bc. The medical use of cannabis was also known in other ancient cultures throughout India, Assyria, Greece, Africa, South America, Egypt, and the Roman Empire.
Cannabis was introduced on a larger scale into Western medicine during the 19th century, primarily by British doctors. They accumulated experience in the use of “Indian hemp” while working in the colonies, recommending it as an appetite stimulant, analgesic, muscle relaxant, anticonvulsant, and hypnotic. In 1839, Dr William Brooke O’Shaughnessy, an Irish physician at the Medical College of Calcutta, published a detailed report “On the preparations of the Indian Hemp or Gunjah.” After performing animal studies, he determined that cannabis preparations were safe and effective in treating rabies, rheumatism, epilepsy, and tetanus. The Ohio Medical Society of Physicians reported in 1860 successful treatment of “stomach pain and gastric distress,” psychosis, chronic cough, gonorrhoea, and neuralgia with cannabis. The plant was difficult to store, its extracts were variable in potency, and the effects of oral ingestion were not constant. Other new drugs were becoming available in the early 1900s with more reliable effects, and cannabis began to be misused for recreational purposes. The American Marijuana Tax Act of 1937 intended to prevent non-medical use, but made cannabis difficult to obtain for medical purposes too, and it was subsequently removed from the US pharmacopoeia in 1942.
In the United States cannabis is now classified as a schedule I drug, regarded as having high potential for abuse, and to be unsafe to take without medical supervision. Recently, several states have legalised the medical use of cannabinoids. In the United Kingdom, cannabis is registered as a schedule I—class C drug. The medical use of cannabinoids is currently restricted to dronabinol (Marinol, synthetic Δ9-tetrahydrocannabinol) and nabilone; these drugs are administered orally as anti-emetics and appetite stimulants for patients with AIDS or on chemotherapy.
Cannabinoid
Cannabinoids and glaucoma
Pharmacology
The cannabis plant has more than 480 chemical constituents. Of these, there is a group of at least 66 compounds that contain only carbon, hydrogen, and oxygen and are known collectively as cannabinoids. The remaining constituents of cannabis include nitrogenous compounds such as amino acids, proteins and glycoproteins, sugars, hydrocarbons, alcohols, aldehydes, ketones, simple acids, fatty acids, esters and lactones, steroids, terpenes, non-cannabinoid phenols, flavonoids, pigments (carotene and zanthophylls), and vitamin K. Terpenes are thought to be responsible for the characteristic odour of cannabis plants.

The main psychoactive constituent of cannabis is the cannabinoid, Δ9-tetrahydrocannabinol (Δ9-THC), the structure of which was determined by Gaoni and Mechoulam in the 1960s.

Most research into the pharmacological properties of plant cannabinoids has focused on this cannabinoid and, indeed, with the exception of cannabinol and cannabidiol, other plant cannabinoids have been subjected to little or no pharmacological research.

It is now generally accepted that Δ9-THC produces many of its effects by acting through cannabinoid receptors of which there are at least two subtypes, CB1 and CB2.8 Both subtypes are coupled through Gi/o proteins, negatively to adenylate cyclase and positively to mitogen activated protein kinase. In addition, CB1 receptors are positively or negatively coupled through Gi/o proteins to certain calcium and potassium channels. CB1 receptors, which were cloned in 1990, are present in brain, spinal cord, and certain peripheral tissues that include lung, heart, urogenital and gastrointestinal tracts, and the eye. Many CB1 receptors are present on central and peripheral neurons, one of their functions being the modulation of neurotransmitter release. CB2 receptors seem to be located especially in cells and tissues associated with the immune system, such as the tonsils, spleen, and different types of leucocytes. One role of these receptors is modulation of cytokine release.
Endogenous agonists for cannabinoid receptors have also been discovered; this system of “endocannabinoids” and receptors constituting what is now generally known as the endocannabinoid system. The endocannabinoids that have been indentified to date are all analogues of arachidonic acid. They include arachidonoyl ethanolamide (anandamide; AEA), 2-arachidonoyl glycerol (2-AG) which bind more or less equally well to CB1 and CB2 receptors, and 2-arachidonyl glyceryl ether (noladin) which is CB1 selective.

AEA behaves as a partial cannabinoid receptor agonist with less CB2 than CB1 efficacy. Within the nervous system, endocannabinoids are synthesised and released by neurons on demand, functioning as neurotransmitters or neuromodulators. There is also evidence that endocannabinoids serve as retrograde synaptic messengers. Following their release, the effects of at least some endocannabinoids are thought to be rapidly terminated by cellular uptake and intracellular enzymatic hydrolysis.
There is evidence too that classic cannabinoids such as Δ9-THC, HU-211, and CBD have antioxidant properties. In addition, Δ9-THC can act through presynaptic CB1 receptors in the CNS to inhibit glutamic acid release and that HU-211 can block glutamate (NMDA) receptors.
As well as showing therapeutic potential as neuroprotective agents, Δ9-THC and CBD have other potential clinical applications; Δ9-THC, for example, is already used in the clinic as an appetite stimulant and anti-emetic. In addition, this cannabinoid will most likely prove to be useful as an anti cancer drug and for the management of pain, and of various kinds of motor dysfunction that include the muscle spasticity, spasm, or tremor associated with multiple sclerosis and spinal cord injury, the tics and psychiatric signs and symptoms of Tourette’s syndrome, and the dyskinesia that is produced by l-dopa in patients with Parkinson’s disease. One other important potential clinical application for cannabinoids, is the management of glaucoma.
Cannabinoids in glaucoma prevention and treatment
Pharmacology of cannabinoids
cannabinoids and glaucoma
In 1971, Hepler and Frank reported a 25–30% IOP lowering effect of smoking marijuana in a small number of subjects. The duration of action of marijuana after smoking was relatively short, about 3–4 hours, and there seemed to be a dose-response relation. Other ocular effects were observed such as conjunctival hyperaemia, reduced tear production, and change in pupil size. Acute systemic side effects induced by marijuana smoking included reduction of systemic blood pressure and tachycardia. Psychotropic effects were very variable and included euphoria or dysphoria, disruption of short term memory, cognitive impairments, sense of time distortion, reduced coordination, and sleepiness.
An earlier report on the effect of smoked marijuana indicated the possibility of tolerance. Thus, the IOP reduction appeared to be inversely related to the duration of marijuana use. In contrast, Dawson et al reported on their ophthalmological findings comparing non-users with long term users of marijuana (10 years or more). After applying the water loading test to both groups, the reduction of IOP associated with marijuana treatment was similar between users and non-users.
Since these early observations numerous studies have been conducted confirming that different cannabinoids, including cannabidiol, cannabigerol, endogenous cannabinoids, and some synthetic cannabinoids, can reduce the IOP when administered systemically and topically. Obviously, smoking of marijuana is not advisable as a long term treatment. In addition to the acute side effects, long term marijuana smoking is associated with emphysema-like lung changes, and possible increase in the frequency of lung cancer. Oral administration has been evaluated. However, there is a poor and variable absorption with this route, at least for the cannabinoid formulations that have been investigated so far.
Cannabinoids and glaucoma
Mechanism of IOP reduction
The mechanism of action of cannabinoids in the human eye is not fully understood. Until recently, the effect of cannabinoids on IOP was assumed to be mediated through the CNS. Studies involving unilateral topical application of cannabinoids showed a large difference between the treated and untreated eye, suggesting a localised action. The experiments of Liu et al revealed evidence pointing in the same direction: bolus administration of Δ9-THC into the cerebral ventricles, as well as ventriculocisternal perfusion with Δ9-THC in rabbits, in contrast with intravenous administration, did not change the IOP. Thus, the main site of action of cannabinoids on IOP is not in the central nervous system.
Pharmacological and histological studies support the direct role of ocular CB1 receptors in the IOP reduction induced by cannabinoids. Straiker et al detected CB1 receptors in ocular tissues of the human eye, including the ciliary epithelium, the trabecular meshwork, Schlemm’s canal, ciliary muscle, ciliary body vessels, and retina. Porcella et al found high levels of CB1 mRNA in the ciliary body. The anatomical distribution of cannabinoid receptors suggests a possible influence of endogenous cannabinoids on trabecular and uveoscleral aqueous humour outflow and on aqueous humour production. In addition to the proved IOP lowering effect of CB1 receptor agonists, Pate et al could antagonise the IOP lowering effect of CP-55,940 (a synthetic CB1 agonist) by pretreating the animals with SR 141716A (a CB1 receptor antagonist). Similarly, Song et al found that the IOP lowering effect of topical WIN-55,212-2 was significantly reduced by topically administered SR141716A.
Using the synthetic cannabinoid WIN-55,212-2 Chien et al could demonstrate an 18% reduction in the aqueous humour production in monkeys but without significant change in the trabecular outflow facility. As this percentage appeared not sufficient to account for the total IOP lowering effect, other additional mechanisms were thought to be involved.
The IOP reducing effect does not seem to be related to a systemic reduction of arterial blood pressure. However, a direct effect on the ciliary processes, and specifically a reduction in capillary pressure, leading to changes in aqueous humour dynamics, has been proposed. Green et al showed that Δ9-THC decreased the secretion of ciliary processes and led to a dilatation of the ocular blood vessels through a possible β adrenergic action. In addition, Sugrue indicated that cannabinoids may inhibit calcium influx through presynaptic channels and in this way reduce the noradrenaline release in the ciliary body, leading to a decrease in the production of aqueous humour. Porcella et al proposed that cannabinoids might be acting as vasodilators on blood vessels of the anterior uvea, thus improving the aqueous humour uveoscleral outflow.
Green et al postulated that some cannabinoids may influence the IOP through a prostaglandin mediated mechanism. For example, topically applied AEA is hydrolysed to arachidonic acid, which is a COX pathway precursor of prostaglandins.
The topical application of the CB2 receptor agonist JWH-133 used in in vivo experiments by Laine et al did not have any effect on IOP compared to vehicle treatments, indicating that CB2 receptor agonists may not be involved in the regulation of IOP.
IOP reduction
CB1 and CB2 receptors
Neuroprotective and vascular actions of cannabinoids
In glaucoma, the final pathway leading to visual loss is the selective death of retinal ganglion cells through apoptosis. Apoptosis is initiated by axonal injury at the optic disc, either by compression and/or by ischaemia. In ischaemia, glutamate is released and activates NMDA receptors. NMDA receptor activation appears to be one of several pathways that result in apoptotic cell death. After activation of NMDA receptors there is an influx of calcium into the cells and free radicals are generated. Substances that prevent this cascade of events and inhibit the retinal ganglion cell death are currently under investigation.
Recent studies have documented the neuroprotective properties of cannabinoids. There is evidence that Δ9-THC can inhibit glutamic acid release by increasing K+ and decreasing Ca2+ permeability and that the synthetic cannabinoid HU-211 can block glutamate (NMDA) receptors. These actions are mediated by presynaptic CB1 receptors. Yoles et al, using a calibrated crush injury to adult rat optic nerve (optic nerve axotomy), showed a beneficial effect of HU-211 on injury induced metabolic and electrophysiological deficits.63 However, the optic nerve crush model may not resemble the mechanisms responsible for glaucomatous nerve damage.
Classic cannabinoids such as Δ9-THC, HU-211, and CBD have antioxidant properties that are not mediated by the CB1 receptor. As a result, they can prevent neuronal death by scavenging toxic reactive oxygen species produced by overstimulation of receptors for the excitatory neurotransmitter, glutamic acid.
Cannabinoids have vasorelaxant properties and so might be able to increase the ocular blood flow. The mediator endothelin-1, produced by vascular endothelial cells, has a significant role in the regulation of local circulation, producing vasoconstriction and being involved in the pathophysiological processes of ischaemic and haemorrhagic stroke, Raynaud’s phenomenon, ischaemic heart disease and pulmonary arterial hypertension, among others. The possible role of endothelin-1 in the pathogenesis of glaucoma has been suggested. For example, patients with open angle glaucoma may have an abnormal increase in plasma endothelin-1 in response to vasospastic stimuli. Mechoulam et al could demonstrate that 2-arachidonoylglycerol, an endogenous cannabinoid, was able to reduce endothelin induced Ca2+ mobilisation, inhibiting vasoconstriction. Thus, cannabinoids may have beneficial properties in ischaemia induced optic nerve damage.
neuroprotective effects
cannabinoids and glaucoma
Future directions
Cannabinoids have the potential of becoming a useful treatment for glaucoma, as they seem to have neuroprotective properties and effectively reduce intraocular pressure. However, several challenges need to be overcome, including the problems associated with unwanted systemic side effects (psychotropic, reduction in systemic blood pressure), possible tolerance, and the difficulty in formulating a stable and effective topical preparation. Some cannabinoids such as HU-211 and cannabidiol do not have psycotropic effects, while maintaining their IOP lowering action, so that further research on these compounds would be desirable. Tolerance may develop after repeated use of cannabinoids. However, tolerance might be beneficial if it develops only or preferentially to unwanted side effects. There has been recent progress in the use of microemulsions and cyclodextrins to overcome the barriers in ocular penetration of topically applied cannabinoids.
Other possible applications of cannabinoids in ophthalmology could be explored. Age related macular degeneration (AMD) is the leading cause of blindness in the United Kingdom. Perhaps the potent antioxidant properties of the cannabinoids may be beneficial in AMD, offering a possible alternative to established antioxidant supplements. Cannabinoids have been shown to inhibit angiogenesis, leading to a decrease in the expression of proangiogenic factors such as VEGF. Evidence suggests that VEGF plays a major part in the development of choroidal neovascularisation in AMD, and clinical trials using anti-VEGF therapies are being conducted. The CB2 receptors are also under intense investigation for their possible immunomodulatory effects. The anti-inflammatory properties of CB2 receptor agonists might also prove to be of therapeutic relevance in different forms of inflammatory eye disease.