Denosumab is a fully human monoclonal antireceptor activator of nuclear factor kappa-B ligand antibody ( moAb ), which inhibits the activity of osteoclasts, resulting in an antiresorptive effect with a significant increase in bone mineral density. It is useful for the treatment of osteoporosis , treatment-induced bone loss, bone metastases, rheumatoid arthritis , multiple myeloma, and giant cell tumor of bone.
Denosumab is designed to target RANKL (RANK ligand), a protein that acts as the primary signal for bone removal. In many bone loss conditions, RANKL overwhelms the body's natural defenses against bone destruction
Postmenopausal osteoporosis results from bone loss and decreased bone strength mediated by an increased rate of bone remodeling secondary to reduced estrogen levels. Remodeling cycles are initiated by osteoclasts, the formation, function, and survival of which depend on RANK ligand. RANKL inhibition therefore represents a novel strategy for reducing remodeling and its effects on fracture risk.
Preclinical evidence from several bone disease models suggests that RANKL inhibition leads to increased bone volume, density, and strength. Denosumab prevents RANKL from binding to its receptor, decreasing osteoclast activity and thereby reducing bone resorption and increasing cortical and trabecular bone mass and strength. It has consistently been reported to reduce bone turnover, increase bone density, and reduce the risk of fracture in clinical studies of postmenopausal women. Phase III head-to-head trials comparing denosumab with the bisphosphonate alendronate reported that denosumab was associated with significantly greater increases in bone density. Eczema as an adverse event and cellulitis as a serious adverse event were more common with denosumab than with placebo.
Preclinical studies defined the role of RANKL in bone remodeling and provided evidence for the therapeutic potential of RANKL inhibition in conditions of bone loss. Clinical studies evaluating RANKL inhibition with denosumab in postmenopausal women have reported significant reductions in vertebral, nonvertebral, and hip fractures, providing evidence compatible with the use of denosumab in postmenopausal women with osteoporosis.
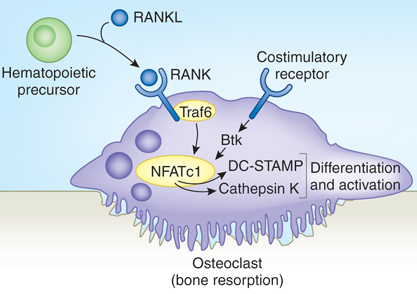
Mechanism
Osteoporotic fractures carry a substantial burden of morbidity and mortality, but pharmacotherapy can prevent such fractures in high-risk individuals. Antiresorptive drugs (e.g. bisphosphonates , oestrogen, denosumab) reduce bone turnover by distinct mechanisms. Denosumab binds the cytokine RANKL (receptor activator of NFκB ligand). RANKL inhibition blocks osteoclast maturation, function and survival, thus reducing bone resorption. In contrast, bisphosphonates bind bone mineral, where they are absorbed by mature osteoclasts, inducing osteoclast apoptosis and suppressing resorption. These differences in mechanism influence both the onset and reversibility of treatment.

Patients with cancer
Denosumab has been developed for use in patients with early-stage and advanced-stage cancer, as well as for the treatment of osteoporosis, and can prevent bone loss and reduce fragility fractures in both types of disease. In the bone metastasis setting, several large phase III studies have shown that denosumab is more effective than bisphosphonates, namely zoledronic acid, in reducing skeletal morbidity arising from a wide range of tumors. In addition, a remarkable activity of denosumab has been demonstrated in giant-cell tumors of the bone. Subsequent studies of denosumab have demonstrated that it can delay bone metastasis in patients with castration-resistant prostate cancer; adjuvant studies in patients with breast cancer are in progress.
Side Effects
The most common side effects include infections of the urinary and respiratory tracts, cataracts , constipation, rashes and joint pain. A small study found a slightly increased risk of cancer and severe infections, but these results did not reach statistical significance. Another trial showed significantly increased rates of eczema and hospitalization due to infections of the skin. It has been proposed that the increase in infections under denosumab treatment might be connected to the role of RANKL in the immune system. RANKL is expressed by T helper cells, and is thought to be involved in dendritic cell maturation.
Denosumab is contraindicated in patients with hypocalcemia, and sufficient calcium and vitamin D levels must be reached before starting on denosumab therapy. Data regarding interactions with other drugs are missing. It is unlikely that denosumab exhibits any clinically relevant interactions.
Similarly to bisphosphonates, denosumab appears to be implicated in increasing the risk of osteonecrosis of the jaw (ONJ) following extraction of teeth or oral surgical procedures.
References
PubMed : Role of RANK ligand and denosumab,2012
PubMed : Denosumab in patients with cancer,2012
Wikipedia : Denosumab