FOLIC ACID: The prevention of neural tube defects
Also called vitamin M, vitamin B9 , folacin or pteroyl-L-glutamic acid.

Folic acid is a water-soluble vitamin of the B Group and it is the only active form of folate absorbed by the body.It is synthetically produced,because it is not naturally found in food,contrary to folate. It is therefore a prodrug.Folic acid is itself not biologically active,but it is converted in the liver in its active form: tetrahydrofolate that can be used and that is able to exploit its biological usefulness.
Food Sources
In foods, folate exists in various combinations of different residue polyglutamic (tri, tetra, penta, hepta) linked to the molecule of folic acid.Foods with a high percentage of folate are: organ meats,like kidney and liver,green leafy vegetables (lettuce, spinach, broccoli),yeast, cereal flakes, legumes and eggs.Its presence is low in fruit and milk. It is also used in fortified foods and supplements used like integrators. The food folates are absorbed mainly in the first intestinal tract, including the duodenum and the ileum, and in the proximal third of the small intestine, although they may be absorbed throughout its length.

Folic Acid Chemistry
Folic acid structure is composed of the union of three molecules: 6-metilpterina acid, p-amino benzoic acid (PABA), and glutamic acid.

Folate enter cells as monoglutamates, but are rapidly modified by addition of four to eight glutamate residues to form long side chains. A group of zinc-dependent intracellular enzymes, the conjugase , are used to obtain folic acid, which is the form normally absorbed from the gut, and then, folic acid is further reduced by the enzyme 5,10- metiltetridrofolato reductase (5,10- MTHFR) in the liver to 5MTHF (5-Methyl-Tedra hydro-folate) that is the active form of the vitamin itself, responsible for significant biological activities known and that is obteined after reduction in diidrofolic acid by diidrofolate reductase. The foletes that are used ase coenzymes and regulatory molecules in the body are all in the reduced form as tetrahydrofolate derivetes. But the capacity of the body to convert folic acid is limited and unmetabolised folic acid has been detected in the systemic circulation following folic acid supplement.
Biological Role
The enzyme 5,10- metiltetridrofolato reductase ( 5,10- MTHFR ) is an enzyme dependent on folic acid that exists in polymorphic form ( genetic polymorphism ). The action of the enzyme 5,10- MTHFR regulates both the phenotypic expression of the DNA metabolism of homocysteine . For this reason folic acid is required for all the reactions of DNA synthesis, repair and methylation , for RNA synthesis, for the metabolism of homocysteine and other important biochemical reactions, particularly during erythropoiesis, the process of formation of red blood cells, and in periods of rapid cell division.For this reason, both children and adults require folic acid to produce normal red blood cells and prevention of anemia.

Folate Deficiency
The folic acid deficiency is very common, especially in underdeveloped countries. The reasons may be related to infectious diseases, drug therapies, pregnancy or malabsorption, and the consequences are problems in the synthesis of DNA and RNA , but also defects in production of bone marrow cells.Folate is required to make red blood cells and white blood cells and folate deficiency may lead to anemia. Folate deficiency limits cell division, erythropoiesis, production of red blood cells, and it is leads to megaloblastic anemia , which is characterized by large immature red blood cells.This pathology results from persistently thwarted attempts at normal DNA replication, DNA repair, and cell division, and produces abnormally large red cells called megaloblasts.The symptoms of folic acid deficiency is also manifested by macrocytic anemia which may be accompanied by leukopenia and thrombocytopenia, abnormal skin and mucous membranes, and gastrointestinal disorders like malabsorption and diarrhea.
From the earliest stages of pregnancy , the product of conception becomes a huge consumer of folate, because of the intense processes of cell proliferation and differentiation. The increase in maternal erythropoiesis contributes to the needs of folic acid during pregnancy in view of childbirth blood volume will be increased by 30-50%. Lack of folic acid can cause congenital malformations ,especially those involving the neural tube defects ( NTD); this term refers to a heterogeneous group of malformations , united by an abnormal closure of the neural tube during the fourth week of embryonic development .The preventive activity against hyperhomocysteinemia folic acid helps also to reduce the cardiovascular risk of the mother, so much so that it has been suggested a preventive role against hypertension in pregnancy and its complications . For this reason , the deficiency of folic acid can increase preeclampsia and eclampsia , recurrent miscarriage , placental abruption , intrauterine growth retardation , low birth weight and intrauterine death .Therefore this deficiency is associated with many pregnancy complications.
Folate and Pregnancy: the importance of folic acid supplementation
Folic acid is essential for the replication of the genetic material,because it plays a key role in the biosynthesis of purines and pyrimidines and amino acids:
The gene encoding the enzyme 5,10- metiltetridrofolato reductase ( 5,10- MTHFR) commonly exhibits a substitution of cytosine with thymine at nucleotide 677, is thus indicated: 677 C> T MTHFR, or C677T MTHFR. The MTHFR gene is located on chromosome 1. The genetic variant C677> T is known to be responsible for a higher incidence of spina bifida or DNT. Therefore it is evident that the 5,10-MTHFR has a critical role in the duplication of the nucleotide biosynthesis. Indeed, with a proper nutritional intake of folic acid, the presence of 5,10-optimal MTHFR protects from the risk of an incorrect development embryogenetic. On the contrary, a low intake of folic acid and consequent reduced production of the enzyme that is involved in the 5,10-MTHFR dall'dUMP proper conversion to dTMP, causes an increase in the incorporation of uracil into DNA with an increase in genomic instability . Therefore, the polymorphism of MTHFR-C677T is heavily responsible for the onset of DTN.
The integration with folic acid does not reset the risk that the product of conception developments defects in neural tube closure , but it significantly reduces.
Therefore it is used as a vitamin supplement in pregnant women. Women who could become pregnant are advised to eat foods fortified with folic acid or take supplements in addition to eating folate-rich foods to reduce the risk of serious birth defects. The World Health Organization (OMS) recommends a daily intake of 400 micrograms in pregnancy in order to prevent the occurrence of spina bifida and 300 micrograms during breastfeeding. Is essential that this assumption beginning one month before conception (to increase reserves) and continues throughout the first trimester of pregnancy. This particular dosage of folic acid is recommended to all the people of childbearing age who do not apply effective contraceptive measures. But Ddoses higher than 0.4 mg of folic acid per day may be specifically recommended only for women who have already had a child affected by defects in neural tube closure , or a family history of such malformations.

Neural Tube defects
Neural tube defects are severe abnormalities of the central nervous system that develop in babies during the first few weeks of pregnancy and that resulting in malformations of the spine, skull, and brain; the most common neural tube defects are spina bifida and anencephaly.
The genesis of neural tube defects NTDs depends on the incomplete closure of the neural tube during fetal development, and defects occurs between 17 and 29 days of gestation , when the complete closure of the neural tube is not yet occured.But often the woman in this period of gestation is not aware of ongoing pregnancy, and for this reason begins the using of folic acid only after the damage has been established embryonic.For this reason in very important the use of massive advertising campaigns that invite to an intake of folic acid as a preventive measure in all women who do not use contraception.
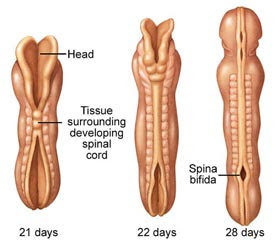
Spina bifida : is a malformation or a birth defect due to incomplete closure of one or more vertebrae, resulting in a malformation of the spinal cord.It is the most common malformation of the peripheral nervous system.It has a prevalence of about one in 8000 newborns, but varies greatly from country to country,and is confired that eating habits can have a significant weight on the manifestation of the disease.
If the event occurs before the closure of the neural tube (the fourth week of embryonic development) we have the open spina bifida, which is incompatible with life, characterized by the absence of skin, vertebral arches, meninges, and exposure of the neural tube.
Otherwise you may have, in order of severity:
*the myelocele (median dorsal cyst covered with skin and containing the malformed bone,without dura mater and vertebral arches);
*the meningocele (median dorsal cyst covered with skin and meninges containing cerebrospinal fluid, bone is in place, but there aren't vertebral arches);
*spina bifida occulta (cracked vertebral arches with normal meninges and skin ,with hypertrichosis, hemangiomas and pigmentation changes).

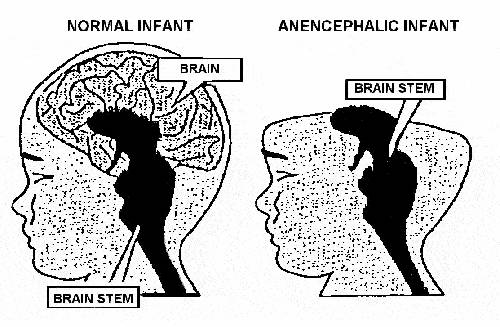
Anencephaly : consists in the absence of a major portion of the brain, skull, and scalp that occurs during embryonic development,usually between the 23rd and 26th day of conception.It is a cephalic disorder that results from a neural tube defect that occurs when the rostral (head) end of the neural tube fails to close.There are many causes of anencephaly and recent studies have shown that the addition of folic acid to the diet of women of child-bearing age may significantly reduce, although not eliminate, the incidence of this pathology.
Studies show the possibility of reduction of this disease through the use of folic acid by 70% in case of recurrence of pregnancy (secondary prevention), in primary prevention this reduction is 62%, while the prevention of perinatal mortality by NTD stands at 13%.Folic acid administration for prevention of neural tube defects in the unborn child should be carried out in the period before conception until the 12th week of gestation and is not effective if treatment is started after the fourth week of pregnancy.It is recommended to continue the supplementation of folate from the beginning of the second quarter, when it ends organogenesis and fetal growth begins, and throughout the remainder of pregnancy to reduce the risk of megaloblastic anemia during the final stage of gestation and the puerperium.
Dietary fortification
Folic acid fortification is a process where folic acid is added to flour with the intention of promoting public health through increasing blood folate levels in the populace.Since the discovery of the link between insufficient folic acid and neural tube defects, governments and health organizations worldwide have made recommendations concerning folic acid supplementation for women intending to become pregnant.
Conclusion
Diet, particularly vitamin deficiency, is associated with the risk of birth defects.Vitamin B9 deficiency plays an important role in the origin of common and severe neural-tube defects and in the congenital heart defects (CHD).Some study indicate that periconceptional folic acid (FA)containing multivitamin supplementation prevents a big proportion (about 90%) of neural tube defects (NTD) as well as a certain proportion (about 40%) of congenital heart defects. Finally the benefits and drawbacks of three main practical applications of folic acid/multivitamin treatment are: dietary intake, periconceptional supplementation and flour fortification.
Folate deficiency and folic acid supplementation: the prevention of neural-tube defects and congenital heart defects, 2013
Women in the reproductive age group should be advised about the benefits of folic acid in addition to a multivitamin supplement during wellness visits (birth control renewal, Pap testing, yearly examination) especially if pregnancy is contemplated.Foods containing excellent acid folic sources are fortified grains, spinach, lentils, chick peas, asparagus, broccoli, peas, Brussels sprouts, corn, and oranges.However, it is unlikely that diet alone can provide levels similar to folate-multivitamin supplementation.Folic acid and multivitamin supplements should be widely available without financial or other barriers for women planning pregnancy to ensure the extra level of supplementation.The recommended strategy to prevent recurrence of a congenital anomaly (anencephaly, myelomeningocele, meningocele, oral facial cleft, structural heart disease, limb defect, urinary tract anomaly, hydrocephalus) is based on acid folic supplementation.A folate-supplemented diet should begin at least three months before conception and continue until 10 to 12 weeks post conception.From 12 weeks post-conception and continuing throughout pregnancy and the postpartum period (4-6 weeks or as long as breastfeeding continues), supplementation should consist of a multivitamin with folic acid (0.4-1.0 mg).The recommended strategy(ies) for primary prevention or to decrease the incidence of fetal congenital anomalies will include a number of options or treatment approaches depending on patient age, ethnicity, compliance, and genetic congenital anomaly risk status.
Pre-conceptional vitamin/folic acid supplementation 2007: the use of folic acid in combination with a multivitamin supplement for the prevention of neural tube defects and other congenital anomalies. 2007
Botto Lorenzo presentation 2003